The ECG
(Note: at the bottom of the page, there are 2 useful video links with ECG examples).
In a resting cardiac muscle cell, there are mostly positively charged ions on the outer surface and negatively charged ions on the inner surface of the cell membrane. Then the cell is in the polarized, resting state. When the cell is stimulated by an excitatory electrical wave, the negative ions pass to the outer surface of the cell and the positively charged ions pass into the cell. This reversal of polarity is called depolarization.
If an electrode is placed so that the depolarization wave has a direction toward the electrode, it will record an upward or positive deflection. This happens because the cells near the electrode have not yet depolarized and so they have a positive membrane potential, and some myocardial cells away from the electrode have depolarized and so they have a negative potential, as the depolarization wave spreads toward the electrode. When all the myocardial cells have depolarized, then there is no potential difference and so the potential difference recorded by the electrode is zero. The opposite phenomena happen during repolarization.
The electrocardiogram (ECG) is the graphic representation of the heart’s electrical activity recorded through electrodes positioned on the body. The electrocardiograph makes the recording of the electrical currents, their magnitude and their direction. It is a sensitive galvanometer. It's deflections are recorded on moving, specially prepared paper.
The ECG paper is covered with a grid of squares. Five small squares on the paper form a larger square. The width of a single small square on the horizontal axis (1mm) represents 0.04 seconds =40 msec (40 milliseconds), with the usual ECG paper speed (25mm/sec) and its height (1mm) on the vertical axis represents 0,1 mV (millivolts) On the horizontal axis a second will be 25 small squares (25 mm) across, or 5 large squares.
The ECG was introduced by Willem Einthoven in 1903,The electrocardiogram is a graphical representation of changes in electrical potential recorded from the body surface. When skeletal muscle is at rest, changes in surface potential reflect cardiac electric activity (propagation of the cardiac depolarization and
then repolarization).
The basic waves of the electrocardiogram (ECG) correspond to the electrical events, which take place during the cardiac cycle.
The P wave represents atrial muscle depolarization. The QRS complex represents ventricular muscle depolarization. Because ventricular muscle mass is much larger than atrial muscle mass, typically the QRS complex is much larger in voltage amplitude than the P wave.
Recorded from multiple points, the QRS complex harbors information about the structure and function of ventricular tissue.
The PR interval, which is the segment from the onset of the P wave to the onset of the QRS complex, represents the delay
between atrial and ventricular depolarization.
The ST segment and T wave (and occasionally the U wave) correspond to the period of ventricular repolarization, a process of electrical recovery that must take place before the ventricle can be depolarized again. The J (junction) point denotes the end of the QRS complex and beginning of the ST segment.
 |
ECG Waves and the ECG paper. From the website ECG Learning Center https://ecg.utah.edu/lesson/12
Licence: Creative commons https://creativecommons.org/licenses/by-nd-nc/1.0/
|
The twelve ECG leads can be described as 12 different positions from which, the electric activity of the heart is recorded and combining the information from multiple leads, with each lead giving a different perspective of the same phenomenon, the spatial orientation of the cardiac electric phenomena is made possible.
Each limb (frontal) lead has its own orientation (or axis) corresponding to the position of its positive and negative poles.A wave of depolarization proceeding along the axis of a lead, toward its positive pole,will result in a maximal positive deflection in that lead, and a less positive deflection in neighboring leads. A wave of depolarization propagating in a direction opposite to the positive pole of a lead (toward its negative pole) will produce a negative wave (a negative deflection).
Lead aVL is –30°.
Lead I is 0°.
Lead II is 60°.
Lead aVF is 90°.
Lead III is 120°.
Lead aVR is –150°
Each of the 6 precordial leads presents its own “perspective,” recording electrical potentials from a different chest surface location.

Limb leads (axis direction)
From http://www.emtresource.com/

Position of precordial leads on the chest
From http://www.nottingham.ac.uk/
The first step in examining an ECG is making sure that the correct name of the patient and date are written on the ECG recording ! The second step is to determine heart rate and rhythm.
In order to understand the ECG, one must know at first the sequence of the electrical activation of the heart. Normally the electrical impulses are generated in the sinoatrial node (SA node) which is the heart's natural pacemaker and consists of a cluster of cells, situated in the upper part of the wall of right atrium, near the origin of the superior vena cava. An electrical signal generated by the SA node is conducted from cell to cell, through the heart. At first the electrical impulse (signal) travels through the atria. Right atrial activation begins before activation of the left atrium, then the impulse is conducted to the left atrium. Both atria undergo activation during much of the middle of the overall atrial activation period and left atrial activation continues after the end of right atrial activation. After atrial activation the impulse reaches the atrioventricular (AV) node, a cluster of cells situated in the center of the heart, between the atria and ventricles. The AV node is characterized by slow conduction of the electrical signal. It serves as a gate, slowing the electrical signal before it is permitted to pass down to the ventricles. This delay ensures that the atria have a chance to fully contract before the ventricles are stimulated. After passing the AV node, the impulse rapidly traverses the bundle of His to enter the bundle branches, and it then travels through the specialized intraventricular conduction paths (Purkinje fibers) to activate ventricular myocardium.
Heart rate determination (pulses per minute, or beats per minute- bpm).
At the usual ECG paper speed (25 mm/s), a distance of 25 mm represents 1 second. Since 1 minute=60 seconds, a distance of 60 x 25 mm=1500 mm represents 1 minute. If the rhythm is regular, a cardiac beat appears at a constant dinstance (D) from the previous one, and so every time the ECG paper runs this distance D, a new cardiac beat appears. Thus, if we measure this distance (D) between two consecutine QRS comlexes in mm, in a situation of a regular heart rate (HR): HR= 1500/D. From this simple rule, and by taking into account that every large square of the ECG paper represents a distance of 5 mm, if the distance D between 2 consecutive R waves is 1 large square, then HR=1500/5=300 bpm. If the distance is 2 large squares HR=150, 3 large squares : HR=100,
4 large squares HR=75, 5 large squares, HR=60, 6 large squares: HR=50, 7 large squares HR=43,
8 large squares : HR=37.5 , 9 large squares HR=33, 10 large squares HR=30, 11 large squares HR=27. It is easy to remember these numbers.
If heart rhythm is irregular (for example in patients with atrial fibrillation) then you can measure how many QRS complexes occur in 6 seconds (in a paper distance of 6 x 25=150 mm= 15 cm=30 large squares) and then multiply this number of QRS comlexes by 10, in order to see how many QRS complexes occur in a minute. Some measure the number of QRS complexes in 3 seconds (15 large squares) and multiply x20. It is essentially the same.
In adults normal heart rate at rest is usually considered to range from 60 to 100 beats per minute (bpm) , but these values are not absolute, because sleeping heart rate may normally fall to about 50 bpm and the normal daytime resting heart rate rarely exceeds 90 bpm. So, from a practical point of view, many doctors consider as normal range of resting heart rate 50-90 bpm. In infants and children heart rate is normally higher.
Normal sinus rhythm is considered to be present when the P wave is positive in I, II, negative in aVR, positive in V2–V6, and positive or biphasic (+/–) in V1, III and posive or biphasic (-/+) in aVL. (this is the morphology of the normal sinus P wave, when the origin of atrial depolarization is from the spread of a sinus electrical impulse).
An abnormal morphology of the P wave can indicate atrial activation from an ectopic focus, or left or right atrial abnormality. With the term atrial abnormality we mean a P wave morphology suggesting dilation of an atrium (hypertrophy of its myocarium may also coexist), or interatrial and intra-atrial conduction delay.
Atrial activation from an ectopic focus is indicated by a P wave with abnormal polarity. For example, a negative P wave in lead
I suggests activation beginning in the left atrium. Inverted P waves in the inferior leads generally indicate a posterior atrial activation
site.
Features indicative of a left atrial abnormality :
Prolonged P wave duration (>120 msec), prominent notching of P wave, with the interval between notches of >40 msec (“P mitrale”), increased duration and depth of the terminal negative portion of P wave in lead V1, so that the area subtended by it >0.04 mm.sec ( > 1 mm2), leftward shift of mean P wave axis to between −30 and −45 degrees. The terminal negative portion of the P wave in lead V1 has a duration > 40 msec or depth > 1mm.
This is lead II. Can you describe any abnormalities ?

Answer
Increased duration of the P wave (> 3mm, i.e > 120 msec) and nospecific ST-T wave changes. The increased duration of the P wave indicates left atrial enlargement.
[This ECG lead is from a 70 years old man who presented with dyspnea with mild exertion and an enlarged cardiac shadow on chest x ray . After testing with echocardiography (which showed left ventricular systolic dysfunction and left ventricular and left atrial enlargement) and coronary arteriography (which showed no significant stenoses of the coronary arteries) he was diagnosed with dilated cardiomyopathy ]
Features indicative of a right atrial abnormality
Peaked P waves with increased amplitude: in lead II >0.25 mV(> 2.5 mm). This is called P pulmonale, because it is often present in cor pulmonale (right heart failure due to severe chronic pulmonary disease), but it can also be noticed in other conditions leading to a dilation of the right atrium.
Prominent initial positive portion of the P wave in lead V1 or V2 >0.15 mV (>1.5 mm).
Increased area under initial positive portion of the P wave in lead V1 >0.06 mm-sec (>1.5 mm2)
Rightward shift of mean P wave axis to more than +75 degrees.
The PR interval is the distance from the beginning of the P wave to the beginning of the QRS complex.
The normal PR interval in adults ranges from 120-200 msec (3-5 mm).
A longer PR interval is seen in cases of atrioventricular (AV) block (delayed or abnormal conduction properties of the AV node, or the bundle of His, or its branches) and shorter PR interval in pre-excitation syndromes and various arrhythmias.
The PR segment is the last part of the PR interval. It is the distance from the end of the P wave to the onset of the QRS and is usually isoelectric (isoelectric in the ECG means a straight line of zero electric potential).
The QRS complex represents ventricular depolarization, which occurs in three consecutive phases that give rise to the generation of three electrical vectors (meaning that each of these 3 phases has a different magnitude and spatial direction of the measured electrical potential). Among the waves constituting the QRS complex, the positive ones are termed R, the negatives are called Q waves when they appear as the initial phase of the QRS, and when they are not the initial waves, the are called S waves. If there are two positive waves (deflections) the first is called R and the second R'. The R, Q, and S, when they are of small amplitude are indicated by a lowercase letter (r,q,s), while when they are larger in size they are denoted by a capital letter. If the QRS consists of a monophasic negative wave, this is called a QS wave.
A normal initial negative wave of ventricular depolarization is called a q wave. Normally it must be narrow (< 40msec) and should not usually exceed 25% of the amplitude of the following R wave, but exceptions exist in leads III, aVL and aVF. If the initial negative deflection is wider or deeper, it is known as a Q wave.
With infarction, depolarization (QRS) changes often accompany repolarization (ST-T) abnormalities, if some time has passed and there is necrosis of sufficient myocardial tissue. This can lead to decreased R wave amplitude or abnormal Q waves in the anterior, lateral, or inferior leads as a result of loss of electrical forces in the infarcted area.
") |
| A normal ECG |
With infarction, depolarization (QRS) changes often accompany repolarization (ST-T) abnormalities, if some time has passed and there is necrosis of sufficient myocardial tissue. This can lead to decreased R wave amplitude or abnormal Q waves in the anterior, lateral, or inferior leads as a result of loss of electrical forces in the infarcted area.
Normal ventricular depolarization has 3 phases. The first phase is the depolarization of the left side of the middle third of the interventricular septum, with a direction from left toward the right side of the septum, with a small resultant electric vector directed rightward and anteriorly. This produces the small initial deflection of the QRS complex. Because depolarization is directed from left to right it produces a small positive (r) wave in leads with a right position, such as avR, V1 and V2 and a small negative wave (septal q wave) in leads with a left orientation, such as I, avL, V5,V6. Then the impulse spreads throughout the apical and free walls of both ventricles in an endocardial to epicardial direction. Because the myocardial mass of the left ventricle is greater than that of the right ventricle, the resultant vector of this main phase of ventricular depolarization is directed leftward and inferiorly. This produces the largest wave of the QRS complex: in leads avR, V1,V2 it is a large negative deflection (S) and in leads I, avL, V5,V6, it is a large positive deflection (R). Finally depolarization arrives at the posterolateral left ventricular wall and the posterobasal septum. This gives rise to a small resultant vector, directed posteriorly and superiorly.
The QRS axis in the frontal plane (the mean direction and amplitude of ventricular electrical activation in this plane) can be assessed from the bipolar and augmented unipolar limb leads (leads I, II, III and avR, avL, avF). By convention, the axis of lead I, toward the left, is called 0 degrees.
The exact method to calculate the axis, would be to calculate the algebric sum of the area of the positive and negative waves of the QRS complex, for each of two leads. If this value is plotted as a vector on the axis of each of the two leads used, the mean frontal plane QRS axis will be the resultant of these 2 vectors. Note that for axis determination the area of a deflection (ECG wave) is more important than its amplitude.This method of axis determination can only be used by a machine (computerized analysis). There are simpler ways to determine (in approximation) the mean frontal plane QRS axis, by applying the following rules:
The axis can be estimated by identifying the limb lead in which the QRS complex is most nearly isoelectric ( the algebric sum of the positive and negative waves is about zero- almost equal positive and negative deflections). The frontal plane axis is perpendicular to that lead. The direction of ventricular depolarization on that frontal plane QRS axis is easily determined, because it must be towards the direction of the leads having a positive net QRS deflection. Another rule is that the QRS axis is approximately the axis of the lead having the most positive algebric sum of the QRS waves (the lead with the most positive net QRS deflection).
A tip for quick analysis of the axis:
If the QRS is net positive in Lead I and in Lead II the axis is normal.
If the net QRS is positive in Lead I but negative in Lead II, there is usually left axis deviation.
If the net QRS is negative in Lead I but positive in Lead II, there is usually right axis deviation.
A frontal plane axis between −30 and +90 degrees is normal, whereas other axes are abnormal in adults.
Right axis deviation: axis between +90 and 180 degrees. Left axis deviation : axis between -30 and -90.
Indeterminate axis : between -90 and 180 (this axis can be extreme left, or extreme right axis deviation). The axis is considered as indeterminate also when positive and negative deflections in all limb leads are equal.
Right axis deviation beyond +90 degrees is often a normal variant in children and adolescents.
Common causes of left axis deviation: left anterior fascicular block (a non- conducting anterior fascicle of the left bundle branch, also called left anterior hemiblock-LAH), inferior wall myocardial infarction, chronic obstructive pulmonary disease (COPD), and Wolff -Parkinson-White syndrome with a posteroseptal accessory pathway.
Causes of right axis deviation include right ventricular hypertrophy or dilation, left posterior fascicular block (also called left posterior hemiblock-LPH), lateral wall myocardial infarction, , Wolff -Parkinson-White syndrome with a left free wall accessory pathway, or a normal variant (in some young people with mild right axis deviation).
In the precordial leads, QRS is normally characterized by progression from an rS pattern= small r and large S (or sometimes QS in V1) in the right precordial leads to a qR (small q, large R) pattern in the left precordial leads. From the right toward the left precordial leads the R wave progressively enlarges and the S wave decreases.
The transitional zone is the lead in which the change of this QRS pattern occurs, where the R and S waves are almost equal in size. Normally the transitional zone is lead V3 or V4.
A shift of the transitional zone to the right (in leads V2 or V1) is called an early transition,or early R wave progression, or counterclockwise rotation of the heart and to the left (in leads V5 or V6) is called delayed transition, or clockwise rotation.
A shift of the transitional zone to the right with an R>S in lead V2 and possibly in lead V1 can occur as a normal variant, or in right ventricular hypertrophy, or in posterior myocardial infarction (MI).
So, the differential diagnosis of a tall R wave (> 7mm or R>S) in the right precordial leads V1,V2 is the following:
RBBB, right ventricular hypertrophy (usually the T wave is negative), posterior MI (usually the T wave is positive in the right precordial leads), Wolff- Parkinson -White (WPW) syndrome with a left sided accessory pathway (because in that case ventricular depolarization begins from the left ventricle through the accesory pathway with a direction from left to right, causing the appearance of a big R wave in right sided leads), rarely a normal variant (in some normal people), Duchenne's muscular dystrophy.
A shift of the transitional zone to the left denoting a delayed or poor R wave progression (clockwise rotation) can occur in lead malpositioning, mild right ventricular hypertrophy as in chronic obstructive pulmonary disease, left bundle branch block (LBBB), left anterior hemiblock (LAH) ,anteroseptal MI, pectus excavatum (the most common congenital chest deformity, with a sunken-concave appearance of the sternum), corrected transposition of the great arteries and congenital absence of the left pericardium.
QRS duration The normal QRS is narrow (normal duration < 100 msec, which means < 2.5 mm), because the His-Purkinje system spreads activation rapidly throughout the ventricles. A prolonged QRS implies slow conduction through the ventricles due to dysfunction ,or circumvention of the His-Purkinje system. This is explained by the fact that conduction through ventricular myocardium is relatively slow.
Aberrancy
Aberrancy refers to patterns of slowed conduction through the ventricles, due to failure of part of the His-Purkinje system.
There are some patterns of aberrancy:
Bundle branch blocks. The bundle of His divides distally in the left and right bundle branches. The left bundle branch further splits into anterior and posterior fascicles. In bundle branch blocks the QRS duration is ≥120 ms (≥ 3 mm wide). This is a feature of both left and right bundle branch block.
A left bundle branch block (LBBB) is characterized by the following : In lead V1 there is a small narrow r wave (if any) and a deep wide S, or a wide QS wave. and in lead V6: a wide monophasic R wave or RsR' pattern (R, small s and a second R). It is also characterized by the absence of septal q waves in leads I, V5, and V6 (the left-oriented leads). In most cases, the ST segment and T wave are discordant with the QRS complex, meaning that the ST segment is depressed and the T wave is inverted in leads with positive QRS waves ( I, aVL, V5, V6), and the ST segment is elevated with an upright T wave in leads with a predominantly negative QRS complex (V1 ,V2).
LBBB occurs in less than 1% of the general population. More commonly it it occurs in people with heart disorders (for example coronary artery disease, dilative cardiomyopathy, hypertensive heart disease, valvular heart disease etc).
However, approximately 10% of the persons with LBBB have no clinically demonstrable heart disease.
LBBB is an ECG pattern with prognostic implications. In persons with or without overt heart disease, LBBB is associated with a higher risk of mortality and morbidity from infarction, heart failure and arrhythmias (including high-grade atrioventricular block) in comparison to the the risk observed in the general population.
A right bundle branch block (RBBB): is characterized by a primarily positive deflection in lead V1, classically with a rSR' pattern, but sometimes with a rsR' or rsr' pattern (“rabbit ears” in V1) and the presence of terminal S waves in leads I and V6 ≥40 msec (1mm) wide. The ST-T waves are (as in LBBB) discordant with the QRS complex : T waves are negative in the right precordial leads (V1,V2) and upright in the left precordial leads (V5,V6) and also in leads I and aVL.
RBBB is a common finding in the general population. Many persons with RBBB have no evidence of structural heart disease.
In people with no manifest cardiac disease, RBBB is not associated with an increased risk of cardiac morbidity or mortality.
In persons with cardiac disease, the presence of RBBB generally suggests more advanced disease (for example this is true for patients with coronary artery disease).
Which are the abnormal findings in this ECG ?

What are the findings in this ECG ?
Which are the abnormal findings in this ECG ?
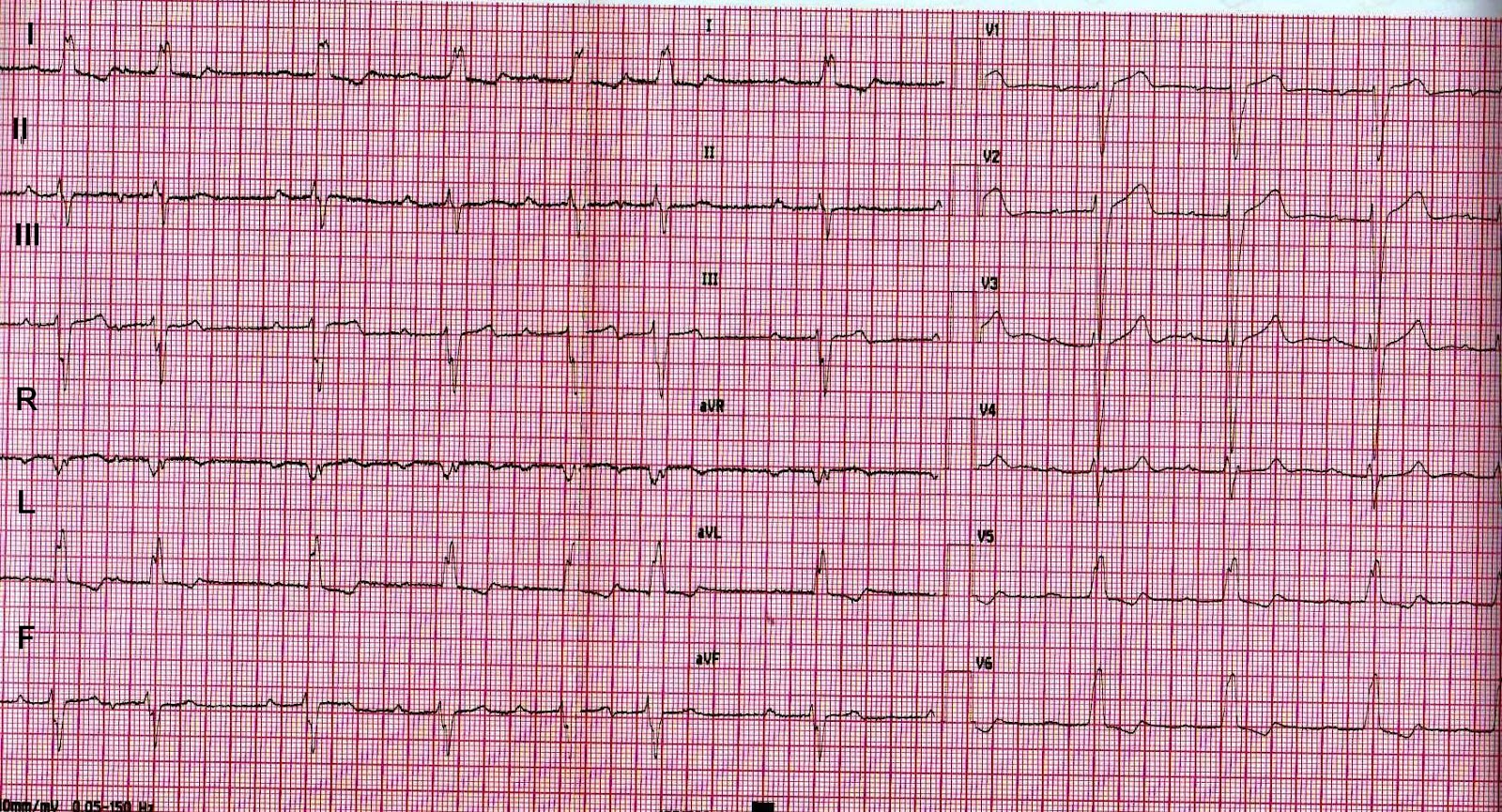
Rhythm : sinus. PR interval prolonged (first degree atrioventricular block).
Some supraventricular premature beats. Left bundle branch block (LBBB). Frontal QRS axis with left deviation.
What are the findings in this ECG ?
 RBBB") |
| Electrocardiogram (ECG) case-1 |
Frontal QRS axis is at about -30 degrees, since the net QRS is almost isoelectric in lead II. This fact alone indicates that the axis can be either -30 degrees, or +150 degrees, but the QRS is positive in lead avL, so the axis cannot be + 150 degrees. It is at -30 degrees. Also note that lead avL has the larger positive algebric sum of the QRS waves.
The Brugada syndrome is a condition, in which an RBBB-like pattern in the ECG (incomplete or complete) with persistent ST segment elevation in the right precordial leads, is associated with susceptibility to ventricular tachyarrhythmias and sudden cardiac death. A number of diagnostic criteria for this entity have been described. The syndrome has been associated with a predisposition for ventricular tachyarrhythmia (polymorphic ventricular tachycardia or ventricular fibrillation) and sudden death. There are three ECG forms of the Brugada syndrome, but only type 1 has been clearly associated with ventricular arrhythmias and a risk of sudden death. Type 1 is characterized by an ST segment elevation ≥ 2mm at the J point (at the junction point of QRS and ST) with the ST segment having the convex upward and forming a downward slope in at least two of the leads V1-V3, with a negative T wave.
Type 2 and type 3 are also characterized by a right bundle branch block morphology (incomplete or complete) with ST segment elevation in the right precordial leads. In type 2, the ST elevation has a concave upward - saddle morphology - and is > 1 mm with a positive or biphasic T wave. Type 3 has an ST pattern similar to type 1 but with an elevation of <2 mm or an ST morphology similar to type 2 but with an elevation <1mm.
Types 2 and 3 are usually normal variants in healthy individuals. However, if there are symptoms (e.g., palpitations- episodes of syncope), then type 2 or 3 poses a diagnostic problem, because it can rarely transiently change into type 1. Then a diagnostic test with flecainide admonistration can be performed, which may in some of these individuals induce the appearance of a type 1 ECG morphology. If administration of flecainide causes this unmasking of type 1, then Brugada syndrome is also diagnosed in these patients, but they have a much lower risk of events than in the spontaneous type 1. The spontaneous type 1 Brugada syndrome has been associated with risk of syncope or sudden death of approximately 0.5% per year.
Asymptomatic individuals with Brugada type 2 or 3 do not require any diagnostic testing.
Brugada syndrome is about 8-9 times more common in men than in women. It results from a mutation of the SCN5A gene coding for a sodium ion channel (INa). Brugada syndrome type 1 may be manifested by either syncope or cardiac arrest (sudden cardiac death) in the third or fourth decade of life (often during sleep) in individuals without stuctural heart disease.

Arrhythmogenic right ventricular cardiomyopathy (AVRC) or arrhythmogenic right ventricular dysplasia is another condition where the ECG often shows an RBBB pattern (complete or incomplete) and inverted T waves in the leads V1-V3 (the leads related to the right ventricle). An epsilon wave can be present i.e. a terminal notch of the QRS (a small wave at the end of the QRS), as a result of slowed intraventricular conduction in an area of the right ventricle. AVRC is a cardiomyopathy caused by a defective gene, characterized by right ventricular systolic dysfunction (global or segmental) due to infiltration of a part of the right ventricle by fbrofatty tissue (in some cases also left ventricular dysfunction) and episodes of monomorphic ventricular tachycardia with an LBBB morphology, which pose a risk of sudden cardiac death.
 |
| Lead V1 with epsilon wave at the end of the QRS. From the ECG of a patient with arrhytmogenic right ventricular cardiomyopathy |

Lead V5 of the same patient with the epsilon wave at the end of the QRS (less prominent than in lead V1).
Another entity characterized by a prolonged QRS interval is pre-excitation. This ECG pattern is caused by the presence of a congenital abnormal pathway of conductive cardiac tissue, between the atria and the ventricles. Such a pathway is called a by-pass tract, or an accessory pathway, through which conduction of electrical impulses can occur, occasionaly resulting in a capacity to form a reentrant circuit, which can function as an arrhythmogenic substrate. The presence of an accessory pathway is an abnormality, since normally the atria and the ventricles are electrically isolated, and electrical contact between them exists only at the atrioventricular node-His bundle conductive tissue. The majority of accessory pathways are capable of conduction in both directions, with retrograde only conduction (from ventricles to atria) occurring in 15% of cases, and antegrade only conduction (only from atria to ventricles) rarely seen.. Accessory pathways that are capable of only retrograde conduction are referred to as "concealed", whereas those capable of antegrade conduction (from the atria down to the ventricles) are referred to as "manifest", because a standard ECG reveals their presence by demontrating pre-excitation. Manifest accessory pathways usually conduct in both anterograde and retrograde directions. In pre-excitation, the ventricles are depolarized by an electrical signal concomitantly conducted through both the accessory pathway and the atrioventricular (AV) node. The part of the ventricle where the accessory pathway connects is the first to depolarize, resulting in a short PR interval and a delta wave on the ECG (a slurring and slow rise of the initial upstroke of the QRS complex). The remaining portion of the ventricular myocardium is depolarized via the normal conductive system (AV node-His bundle-Purkinje fibers) Thus, the typical ECG features of preexcitation include: A short PR interval <120 ms, a slurring and slow rise of the initial upstroke of the QRS complex (called a delta wave), a wide QRS complex > 120 ms and ST segment-T wave changes directed opposite the delta wave and QRS complex, (reflecting altered depolarization).
Accessory pathways usually can conduct rapidly (i.e. an electrical impulse moves through the pathway at a fast velocity), but they frequently have a longer refractory period than the AV node (Refractory period is the time after tissue is activated by an electrical impulse, during which it cannot conduct another impulse).
Although a by-pass (accessory pathway) tract can result in arrhythmias, not all patients with a by-pass tract or with preexcitation manifest tachyarrhythmias. The diagnosis of Wolff-Parkinson-White (WPW) syndrome is reserved for patients who have both preexcitation on the ECG and also manifest tachyarrhythmias. (also see chapter on arrhythmias). The most common arrhythmia encountered in people with pre-excitation is atrioventricular reentry tachycardia (AVRT),a reentrant supraventricular arrhythmia. In AVRT, the AV node is one portion of the reentrant circuit and the other portion is the accessory pathway (most usually the accessory pathway forms the retrograde limb of the circuit, by conducting from the ventricles to the atria, but rarely it forms the antegrade limb).
Bibliography
Sethi KK, Dhall A ,et al. WPW and Preexcitation Syndromes. JAPI supplement 2007;55: 10-15
Fascicular blocks typically prolong the QRS slightly, QRS duration is < 120 ms and cause an abnormal frontal QRS axis (see the section on the frontal plane axis of the QRS)
In Left anterior fascicular block or left anterior hemiblock (LAFB or LAH) there is left axis deviation. There is a qR pattern in lead aVL and the time to peak R wave in aVL ≥45 msec. Left anterior fascicular block also can produce some changes in the precordial leads: Leads V4 - V6 commonly show deep S waves. Damage to the left anterior fascicle is very common because of its delicate nature. Left anterior fascicular block is common in persons without cardiac disease, but it is also common in various cardiac pathologic conditions.
In Left posterior fascicular block or left posterior hemiblock (LPFB or LPH) there is a right axis deviation
A left posterior fascicular block is relatively rare, since the posterior fascicle is wider and highly branched, and loss of all the branches is uncommon. Besides right axis deviation, there is an rS pattern in leads I and aVL and qR complexes in the inferior leads.
A left posterior fascicular block can occur in patients with any cardiac disease, but is unusual in people without cardiac disease.
A man 60 years old with a history of paroxysmal atrial fibrillation and hypertension. Can you list 4 abnormalities in his ECG ?

Sinus rhythm. Abnormalities : 1 supraventricular premature beat, 1 ventricular premature beat, prolonged sinus P wave (see lead II) consistent with possible left atrial enlargement and left anterior fascicular block or left anterior hemiblock (LAFB or LAH)
----------------------------------------------------------------
A 62 years old male with mechanical prosthetic valves in the aortic and mitral position (because of rheumatic valve disease) on anticoagulation treatment with acenocoumarol, states that in the last month he experienced episodes of a transient discomfort (felt like pressure and vague pain). The discomfort was rather diffuse, on the central area of the chest, lasting a few minutes, appearing with physical activity (brisk walking) and resolving with discontinuation of activity. Physical examination revealed no significant findings. His ECG is shown. What is the most probable cause of the patient's symptoms? What does the ECG show ? Is the ECG helpful for the diagnosis in this case?A man 60 years old with a history of paroxysmal atrial fibrillation and hypertension. Can you list 4 abnormalities in his ECG ?

Sinus rhythm. Abnormalities : 1 supraventricular premature beat, 1 ventricular premature beat, prolonged sinus P wave (see lead II) consistent with possible left atrial enlargement and left anterior fascicular block or left anterior hemiblock (LAFB or LAH)
----------------------------------------------------------------

ANSWER
The history alone is sufficient to lead to the most probable diagnosis in this case. The description of the symptoms is typical for effort angina, and the most probable underlying condition in males of this age group is coronary artery disease (CAD).
The ECG shows features of preexcitation, as in Wolff-Parkinson-White (WPW) syndrome : A short PR interval <120 ms, a slurring and slow rise of the initial upstroke of the QRS complex (called a delta wave), a wide QRS complex > 120 ms
and ST segment-T wave changes directed opposite the delta wave and QRS complex, (reflecting altered depolarization). These ECG findings are of course urelated to the patient's symptoms and can in many cases obscure ischemic ECG changes (posing difficulties in the diagnosis of CAD, especially with an ECG exercise test, which would be an innappropriate diagnostic test for CAD in a patient with a preexcited ECG).
The patient had a coronary angiography and he was diagnosed with CAD ( he had a severe stenosis of the left main coronary artery).
A nonspecific intraventricular conduction delay is a condition characterized by widening (prolongation) of the QRS that does not conform to a specific pattern.
Low QRS voltage: Low ampitude of the whole QRS in limb leads is defined as the sum of the absolute amplitude of the R and S wave in every limb lead 5mm (0.5mV) or less and in the precordial leads a sum of 10mm or less in every precordial lead.
Causes of low QRS voltage include obesity, chronic obstructive pulmonary disease, a large pleural effusion, pericardial effusion , pneumothorax, dilative or ischemic cardiomyopathy.
In dilative cardiomyopathy sometimes we have the following characteristic findings: A relatively low whole QRS amplitude in limb leads (<8mm), with a large QRS amplitude in the precordial leads (the sum of S wave in V1 or V2 and the R wave in V5 or V6 is > 35mm) and slow R wave progression in the precordial leads (R<S in leads V1-V4).
The T wave, together with the preceding ST segment, is formed during ventricular repolarization.
The ST segment normally is isoelectric, or shows only a slight depression (< 0.5 mm).
With infarction, depolarization (QRS) changes often accompany repolarization (ST-T) abnormalities, if some time has passed and there is necrosis of sufficient myocardial tissue. This can lead to decreased R wave amplitude or abnormal Q waves in the anterior, lateral, or inferior leads as a result of loss of electrical forces in the infarcted area.
The ECG of a male patient, 65 years old, who complained of retrosternal pain since about half an hour, with perspiration. What is: 1) the diagnosis and 2) the proposed treatment?

Answer
1.Acute anterolateral ST elevation myocardial infarction (STEMI). Note the ST segment elevation in the anterior leads V1-V4 and the lateral leads V5,V6 and I and a mirror ST depression in leads III and aVF.
2. Nitrates (if there is no hypotension), aspirin, clopidogrel loading dose (or ticagrelor loading dose),morphine, oxygen administration (particularly if the hemoglobin saturation is below normal) and as soon as possible primary angioplasty (if it can be done within 120 minutes) or thrombolysis if primary angioplasty cannot be performed promptly (at most within 120 minutes). Also heparin (standard or low molecular weight heparin), a beta-blocker (if there is no bradycardia or hypotension), an ACE inhibitor (if there is no hypotension) and a statin.
A man 52 years old, with crushing substernal chest pain. What is the diagnosis and which artery is probably responsible? (the ECG is courtesy of Dr Najeebullah Sajid (facebook group CARDIOCARE)

The rhythm is sinus. There is ST elevation in the lateral leads (I, avL, V5, V6) , thus this is a lateral acute myocardial infarction (STEMI). There is also ST depression in V1 and V2 which can be attributed to an acute posterior myocardial infarction. (If we had placed an ECG lead at the patient's back, facing the posterior wall, this lead would show an ST-segment elevation). ST depression in leads III and avF is due to a mirror image of the ST elevation in the lateral leads. Often in an acute STEMI there is a mirror image of ST depression in leads having a different or opposite direction than the leads which are close to the site of the infarction. Conclusion: An acute ST-elevation myocardial infarction (STEMI) of the lateral and posterior wall (territory of the left circumflex coronary artery-LCX, which is the occluded artery in this case). Emergency reperfusion with a PCI or thrombolysis is required for this patient.
Female 70 years old diabetic with dizziness, fatigue, sweating, and vomiting since one hour. On physical examination she has jugular vein distension and hypotension (systolic blood pressure 85 mmHg) What is the cause of hypotension? What should be the treatment and what medication is contraindicated?

Answer:
The ECG shows sinus rhythm (there are normal P waves) and ST elevation in the inferior leads (II, III, avF) and the right precordial leads V3R, V4R . There is also "mirror" ST depression in leads I, avL. Therefore, the diagnosis is an acute inferior myocardial infarcion (MI) with acute right ventricular infarction . This type of infarction is due to an occlusion in the right coronary artery (RCA). In this case, the patient did not have the pain of the infarction, probably due to diabetic neuropathy (typically she should feel pain or pressure on the central area of the chest, sometimes also at the epigastrium). Perspiration (sweating), fatique and nausea are common nonspecific symptoms accompanying an acute MI. Hypotension and jugular vein distention are common clinical findings in a right ventricular (RV) infarction, due to the impairment of the RV contractile function. Right ventricular dysfunction causes both the reduction in cardiac output (leading to hypotension) and the increase in RV diastolic pressure with a consequent increase in right atrial and central venous pressure (leading to jugular venous distention).
In such cases, of an acute inferior MI accompanied by an RV infarction and hypotension, intravenous saline (0.9 % NaCl solution) is administered to raise blood pressure, antiplatelet and anticoagulant treatment (as in every acute MI) and promptly (without delay) urgent reperfusion with angioplasty and stenting. If primary angioplasty within less than 90 minutes is not possible, then thrombolysis is administered. Nitrates are containdicated in an acute RV infarction, even if hypotension is not present.
A woman 60 years old presenting with pain on the substernal area and the precordium since 12 hours. The pain increases when lying flat and with deep inspiration. What are the ECG findings and what is the proposed diagnostic testing and probable treatment ?
Answer
The ECG shows sinus rhythm and normal QRS frontal axis. There is PR segment depression (note that the PR segment is at a lower level than the TP segment) in many leads (II, aVF, V2-V6) and PR segment elevation in avR. There is also a mild ST segment elevation (concave upward) in some leads (V2-V5, II). These ECG findings and the characteristics of the pain raise a suspicion of acute pericarditis, although the ECG is not completely typical (usually in acute pericarditis the concave upward ST segment elevation is more diffuse-present in more leads- and more prominent, than in this ECG). However the ECG , as mentioned above, shows some features suggestive of acute pericarditis. Testing should include the usual general blood tests plus c-reactive protein (CRP) and echocardiography. In this case, blood tests showed an elevated leukocyte count (13000/ μL) and moderately elevated CRP. Cardiac troponin test was negative. Echocardiography in this case showed a small pericardial effusion. Treatment of acute pericarditis should be with non steroidal anti-inflammatory drugs (NSAIDs: usually aspirin, ibuprofen, indomethacin, or naproxen) at least for about 2 weeks usually in combination with a drug protective for the stomach (e.g. omeprazol, lansoprazol, pantoprazol, or ranitidine). A full-dose NSAID should be maintained until normalization of the C-reactive protein (CRP) followed by gradual tapering of the drug for another 1-2 weeks to prevent early reoccurrence. In more severe cases of acute pericarditis (e.g. with severe pain showing a delayed response to treatment with a NSAID, or with a moderate to large pericardial effusion), or in reccurent pericarditis concomitant administration of colchicine (combined with the administration of NSAIDS) can improve treatment effectiveness and reduce the posibility of further recurrences. (See chapter "Acute pericarditis -pericardial effusion").
QTc=QT/√RR
Bazett’s formula works well at heart rates within the normal range but overcorrects at high rates (so at high rates it gives a QTc relatively greater than real) and undercorrects at low rates (estimating again a QTc relatively greater than real). The upper limit of a normal QTc is in men 0.45 second (450 msec) and in women 0.46 second (460 msec) . Patients with a congenital or acquired prolonged QTc, especially if it is markedly prolonged (480 msec or more) may be at risk for torsades de pointes ventricular tachycardia.A short QTc interval (<390 msec) is rare, but it also carries an increased risk of malignant ventricular arrhythmias.
Hypercalcemia and hypocalcemia predominantly alter the action potential duration and so they influence the QT interval. Hypercalcemia (increased calcium concentration in the blood) results in a shortened QT interval. Severe hypercalcemia also can be associated with decreased T wave amplitude, T wave notching, or inversion and sometimes with a high takeoff of the ST segment in leads V1 and V2. Hypocalcemia ( reduced calcium concentration in the blood) causes prolongation of the QT interval, due to prolongation of the ST segment.
The point at the end of the QRS complex and the beginning of the ST segment is called the junctional point (J point) and is normally at or near the isoelectric line.
The T wave normally has an ascending slope with slower inscription than the descending slope. The polarity of the T wave normally is essentially the same as the net polarity of the preceding QRS complex because normally the mean vector of the T wave has roughly the same orientation as the mean QRS vector. The T wave normally is generally positive in all leads except aVR, but there are some normal exceptions :
The T wave normally has an ascending slope with slower inscription than the descending slope. The polarity of the T wave normally is essentially the same as the net polarity of the preceding QRS complex because normally the mean vector of the T wave has roughly the same orientation as the mean QRS vector. The T wave normally is generally positive in all leads except aVR, but there are some normal exceptions :
1) In lead V1 the T wave often is negative, flattened or only slightly positive
2) Also in some normal people the T wave can be flattened or slightly negative in leads V2, III and aVF.
2) Also in some normal people the T wave can be flattened or slightly negative in leads V2, III and aVF.
3) In children, a negative T wave is normal when seen in the right precordial leads V1-V3 and occasionally V4 (pediatric repolarization pattern). This pattern usually changes with puberty of after puberty to the normal adult pattern with positive T waves in all the precordial leads (except V1 which may have a negative T wave. Some normal adults may have a negative T wave also in V2).
4) Some normal adults have a persistent juvenile T wave inversion pattern, with negative T waves in the right and middle precordial leads (typically in V1-V3, occasionally also V4 ).
4) Some normal adults have a persistent juvenile T wave inversion pattern, with negative T waves in the right and middle precordial leads (typically in V1-V3, occasionally also V4 ).
A U wave is a small wave, which is occasionally present, after the T wave (a small rounded wave ≤1 mm that follows the T wave). Normally it is smaller than the preceding T wave and has the same polarity. An abnormal increase in U wave amplitude is most commonly due to some antiarrhythmic drugs (such as ibutilide, dofetilide, sotalol, quinidine, procainamide, or disopyramide) or hyperkalemia (elevated serum potasium concentration).
U wave inversion is a sign of ischemia and it can be sometimes the earliest ECG sign of an acute coronary syndrome, although it is not often found. Transient inversion of the precordial U waves induced by exercise, is a sign of ischemia and has been correlated with a significant stenosis of the left anterior descending (LAD) coronary artery.
Abnormalities of the ST segment and the T wave are often characterized as nonspesific especially if these abnormalities are minor. There are also some prominent ST-T wave abnormalities which are considered diagnostic for important clinical disorders, e.g. a typical ECG pattern suggestive of transmural ischemia with ST elevation (which may or may not be preceded by tall "hyperacute" T waves ) or subendocardial ischemia with ST segment depression or T wave inversion in the appropriate clinical situation, see below.
In the case of minor ST-T wave abnormalities, the physician should decide if they have diagnostic significance or not, depending on the clinical situation (the patient's history and physical findings e.g. symptoms, risk factors etc.). Minor ST and T wave abnormalities are usually not considered important (except if the patient has many risk factors for coronary artery disease or symptoms). In some cases they appear in people with a normal heart (without any cardiac disease), whereas in some other cases they are associated with left ventricular diastolic dysfunction (eg. in hypertensive individuals) or with left ventricular hypertrophy or with subclinical coronary artery disease (coronary artery disease that has not yet resulted in symptoms). T wave inversion has a higher probability to be due to myocardial ischemic disease or another pathologic condition when it is ≥ 2 mm and ST depression when it is > 0.5 mm.
Usually most physicians ignore minor ST-T wave abnormalities in people without significant cardiovascular risk factors and without symptoms on physical exertion. If significant cardiovascular risk factors or symptoms with physical exertion are present, then further testing is usually indicated (e.g. echocardiography, exercise ECG testing or stress testing with imaging such as myocardial scintigraphy or stress echocardiography).
Etiology: Minor T wave changes are non-specific, because they have many different etiologies. Prominent T wave abnormalities also have multiple etiologies but in some cases they provide a more specific pattern. They can occur with:
Anxiety -heightened adrenergic state (influences of the sympathetic nervous system)
Hyperventilation (it can cause ST segment depression)
Changes in position
Drinking hot or cold beverages
After a meal
As a normal variant
(The ST or T wave abnormalities in the above cases, when present, are usually minor- not very prominent)
The athletic heart (a constellation of findings present in people that undergo intensive training which is not due to any heart disorder). Some normal athletes have prominent T wave inversions
CNS events (stroke, intracranial hemorrhage) can cause ST-T wave changes, sometimes prominent.
Hyperkalemia can cause tall, narrow peaked T waves.
Hypokalemia can cause low amplitude or inverted T waves
Ischemia can cause mild ST-T wave changes such as low amplitude T waves or small inverted T waves. It can also cause prominent abnormalities such as deep inverted or biphasic T waves, prominent ST elevation or ST depression (usually horizontal or downsloping)
Myocardial hypertrophy either secondary to hypertension or aortic stenosis, or associated with hypertrophic cardiomyopathy can cause ST-T wave abnormalities (minor or prominent) with or without the voltage criteria of left ventricular hypertrophy. Typically, apical hypertrophic cardiomyopathy is associated with prominent (deep) T wave inversions in the precordial leads. Left ventricular hypertrophy typically is associated with the ECG pattern of left ventricular strain in leads facing the left ventricle (I, avL, V5, V6). This pattern is characterized by ST segment depression (usually downsloping) and T wave inversion (negative T wave). Left ventricular strain is a term meaning that the ECG abnormality results from the increased workload of the left ventricle usually due to pressure overload (e.g in hypertension or significant stenosis of the aortic valve).
Other cardiomyopathies such as Tako-tsubo cardiomyopathy (stress cardiomyopathy) and arrhytmogenic right ventricular cardiomyopathy can be associated with T wave inversions (see chapter on cardiomyopathies- link The Cardiomyopathies)
Myocarditis can be associated with ST segment elevation, diffuse T wave inversion or arrhythmias. It is an inflammatory disease of the myocardium that more commonly results from a viral infection but it can also result from mycoplasma infection, drugs and toxins or diseases which can lead to an immune-mediated myocardial inflammation such as systemic lupus erythematosus, scleroderma, Kawasaki's disease. It can cause systolic heart failure.
In pericarditis after the normalization of the ST segment, which is initially elevated, a phase of diffuse T wave inversion follows.
Pericarditis is an inflammation of the pericardium, caused by a viral (usually), or a bacterial (rare) infection, immunologic reactions (e.g. autoimmune disease, postpericardiectomy syndrome after heart surgery), uremia, malignancies etc.
Global idiopathic T wave inversion: The rare occurence of negative T waves in all chest leads (V1-V6) in an adult without evidence of heart disease.
Right ventricular strain Pulmonary embolism, pulmonary hypertension or right ventricular hypertrophy can cause inverted T waves with or without ST depression in leads that have an orientation roughly toward the right ventricle due to right ventricular strain (meaning right ventricular pressure overload which adversely affects its function). These are the right precordial leads (V1-V3 and occasionally V4) and the inferior leads II, III, aVF (among these inferior leads, the ST-T wave abnormality is often more pronounced in lead III because this the most rightward facing lead).
Secondary ST-T wave abnormalities These are ST-T wave changes solely due an alteration in the sequence of ventricular activation. The ST segment and the T wave have a direction opposite to the QRS, e.g. there is ST depression and a negative T wave in leads with a positive net QRS). This is observed in bundle branch blocks, Wolff-Parkinson-White (WPW) syndrome, paced ventricular beats and ventricular arrhythmias (premature ventricular beats and ventricular tachycardia).
"Memory T waves" are inverted T waves that may appear after periods of intermittent rate dependent left bundle branch block, preexcitation (WPW pattern), or ventricular pacing.
A general approach to the patient with nospecific ST-T wave abnormalities.
The patient with ST- T wave abnormalities should be questioned regarding past or present symptoms of myocardial ischemia including chest pain. In some patients a history of athletic training, or symptoms and signs of stroke could explain the electrocardiographic abnormality. Physical examination may reveal hypertension, signs of valve disease or signs of cardiomyopathy in some patients with T wave abnormalities. Echocardiography is generally a very helpful test to diagnose left ventricular hypertrophy, a cardiomyopathy or valve disease.Blood tests should also be obtained including electrolytes (potassium , sodium, calcium magnesium), glucose, BUN (blood urea nitrogen), creatinine and also a complete blood count to look for anemia.
Prominent ST-T wave abnormalities raise more concerns and they also have many etiologies. Some of these etiologic conditions are emergencies, such as the acute coronary syndrome (STEMI or non-STEMI), other conditions are chronic but important, such as hypertrophic cardiomyopathy, but there is also a condition termed idiopathic T wave inversion, where despite the presence of prominent T wave inversion, diagnostic tests do not reveal an underlying heart disease.
Some important abnormalities of the ST segment and the T wave are listed below.
U wave inversion is a sign of ischemia and it can be sometimes the earliest ECG sign of an acute coronary syndrome, although it is not often found. Transient inversion of the precordial U waves induced by exercise, is a sign of ischemia and has been correlated with a significant stenosis of the left anterior descending (LAD) coronary artery.
Abnormalities of the ST segment and the T wave are often characterized as nonspesific especially if these abnormalities are minor. There are also some prominent ST-T wave abnormalities which are considered diagnostic for important clinical disorders, e.g. a typical ECG pattern suggestive of transmural ischemia with ST elevation (which may or may not be preceded by tall "hyperacute" T waves ) or subendocardial ischemia with ST segment depression or T wave inversion in the appropriate clinical situation, see below.
In the case of minor ST-T wave abnormalities, the physician should decide if they have diagnostic significance or not, depending on the clinical situation (the patient's history and physical findings e.g. symptoms, risk factors etc.). Minor ST and T wave abnormalities are usually not considered important (except if the patient has many risk factors for coronary artery disease or symptoms). In some cases they appear in people with a normal heart (without any cardiac disease), whereas in some other cases they are associated with left ventricular diastolic dysfunction (eg. in hypertensive individuals) or with left ventricular hypertrophy or with subclinical coronary artery disease (coronary artery disease that has not yet resulted in symptoms). T wave inversion has a higher probability to be due to myocardial ischemic disease or another pathologic condition when it is ≥ 2 mm and ST depression when it is > 0.5 mm.
Usually most physicians ignore minor ST-T wave abnormalities in people without significant cardiovascular risk factors and without symptoms on physical exertion. If significant cardiovascular risk factors or symptoms with physical exertion are present, then further testing is usually indicated (e.g. echocardiography, exercise ECG testing or stress testing with imaging such as myocardial scintigraphy or stress echocardiography).
Etiology: Minor T wave changes are non-specific, because they have many different etiologies. Prominent T wave abnormalities also have multiple etiologies but in some cases they provide a more specific pattern. They can occur with:
Anxiety -heightened adrenergic state (influences of the sympathetic nervous system)
Hyperventilation (it can cause ST segment depression)
Changes in position
Drinking hot or cold beverages
After a meal
As a normal variant
(The ST or T wave abnormalities in the above cases, when present, are usually minor- not very prominent)
The athletic heart (a constellation of findings present in people that undergo intensive training which is not due to any heart disorder). Some normal athletes have prominent T wave inversions
CNS events (stroke, intracranial hemorrhage) can cause ST-T wave changes, sometimes prominent.
Hyperkalemia can cause tall, narrow peaked T waves.
Hypokalemia can cause low amplitude or inverted T waves
Ischemia can cause mild ST-T wave changes such as low amplitude T waves or small inverted T waves. It can also cause prominent abnormalities such as deep inverted or biphasic T waves, prominent ST elevation or ST depression (usually horizontal or downsloping)
Myocardial hypertrophy either secondary to hypertension or aortic stenosis, or associated with hypertrophic cardiomyopathy can cause ST-T wave abnormalities (minor or prominent) with or without the voltage criteria of left ventricular hypertrophy. Typically, apical hypertrophic cardiomyopathy is associated with prominent (deep) T wave inversions in the precordial leads. Left ventricular hypertrophy typically is associated with the ECG pattern of left ventricular strain in leads facing the left ventricle (I, avL, V5, V6). This pattern is characterized by ST segment depression (usually downsloping) and T wave inversion (negative T wave). Left ventricular strain is a term meaning that the ECG abnormality results from the increased workload of the left ventricle usually due to pressure overload (e.g in hypertension or significant stenosis of the aortic valve).
Other cardiomyopathies such as Tako-tsubo cardiomyopathy (stress cardiomyopathy) and arrhytmogenic right ventricular cardiomyopathy can be associated with T wave inversions (see chapter on cardiomyopathies- link The Cardiomyopathies)
Myocarditis can be associated with ST segment elevation, diffuse T wave inversion or arrhythmias. It is an inflammatory disease of the myocardium that more commonly results from a viral infection but it can also result from mycoplasma infection, drugs and toxins or diseases which can lead to an immune-mediated myocardial inflammation such as systemic lupus erythematosus, scleroderma, Kawasaki's disease. It can cause systolic heart failure.
In pericarditis after the normalization of the ST segment, which is initially elevated, a phase of diffuse T wave inversion follows.
Pericarditis is an inflammation of the pericardium, caused by a viral (usually), or a bacterial (rare) infection, immunologic reactions (e.g. autoimmune disease, postpericardiectomy syndrome after heart surgery), uremia, malignancies etc.
Global idiopathic T wave inversion: The rare occurence of negative T waves in all chest leads (V1-V6) in an adult without evidence of heart disease.
Right ventricular strain Pulmonary embolism, pulmonary hypertension or right ventricular hypertrophy can cause inverted T waves with or without ST depression in leads that have an orientation roughly toward the right ventricle due to right ventricular strain (meaning right ventricular pressure overload which adversely affects its function). These are the right precordial leads (V1-V3 and occasionally V4) and the inferior leads II, III, aVF (among these inferior leads, the ST-T wave abnormality is often more pronounced in lead III because this the most rightward facing lead).
Secondary ST-T wave abnormalities These are ST-T wave changes solely due an alteration in the sequence of ventricular activation. The ST segment and the T wave have a direction opposite to the QRS, e.g. there is ST depression and a negative T wave in leads with a positive net QRS). This is observed in bundle branch blocks, Wolff-Parkinson-White (WPW) syndrome, paced ventricular beats and ventricular arrhythmias (premature ventricular beats and ventricular tachycardia).
"Memory T waves" are inverted T waves that may appear after periods of intermittent rate dependent left bundle branch block, preexcitation (WPW pattern), or ventricular pacing.
A general approach to the patient with nospecific ST-T wave abnormalities.
The patient with ST- T wave abnormalities should be questioned regarding past or present symptoms of myocardial ischemia including chest pain. In some patients a history of athletic training, or symptoms and signs of stroke could explain the electrocardiographic abnormality. Physical examination may reveal hypertension, signs of valve disease or signs of cardiomyopathy in some patients with T wave abnormalities. Echocardiography is generally a very helpful test to diagnose left ventricular hypertrophy, a cardiomyopathy or valve disease.Blood tests should also be obtained including electrolytes (potassium , sodium, calcium magnesium), glucose, BUN (blood urea nitrogen), creatinine and also a complete blood count to look for anemia.
Prominent ST-T wave abnormalities raise more concerns and they also have many etiologies. Some of these etiologic conditions are emergencies, such as the acute coronary syndrome (STEMI or non-STEMI), other conditions are chronic but important, such as hypertrophic cardiomyopathy, but there is also a condition termed idiopathic T wave inversion, where despite the presence of prominent T wave inversion, diagnostic tests do not reveal an underlying heart disease.
Some important abnormalities of the ST segment and the T wave are listed below.
Transmural ischemia : An ST segment elevation occurring in leads representing an identifiable coronary distribution (e.g., inferior, anterior, lateral), suggests acute and ongoing myocardial transmural ischemic injury, as seen in acute coronary occlusion (myocardial infarction). It can also occur in a case of coronary artery spasm (a condition called variant angina or Prinzmetal's angina), see the first case in the chapter on coronary artery disease (link :Coronary artery disease)
In an appropriate clinical setting (acute symptoms raising suspicion of an acute coronary syndrome) coronary occlusion causing transmural myocardial ischemia (an ST elevation myocardial infarction STEMI) is diagnosed by the following ECG findings:
1) In leads V2 -V3, ST segment elevation of 2 mm (0.2 mV) or more at the J point in men, or 1.5 mm (0.15 mV) or more in women in the absence of left ventricular hypertrophy, or
2) in two or more other contiguous chest or limb leads the presence of an ST elevation of 1 mm (0.1 mV) or more. In such patients, emergency reperfusion (primary angioplasty or fibrinolysis) should be performed, unless there is a contraindication.
3) Another diagnostic ECG criterion for a STEMI, if compatible symptoms are also present (i.e., in the appropriate clinical setting) is a new or presumably new LBBB (which may obscure ST elevation analysis). In this case emergency reperfusion is also indicated.
4) Another type of STEMI (in which prompt emergency reperfusion is performed, as for any STEMI) is a true posterior myocardial infarction (MI). True posterior MI in the acute phase presents ST depression in leads V1, V2 (and sometimes also in V3, V4). This is a mirror-image of ST elevation in the posterior leads V7-V9 and is usually caused by an acute infarction in the territoty of a non dominant left circumflex (LCX) coronary artery. In case of suspicion, extending the ECG to left posterior leads V7 -V9 increases sensitivity (also with excellent specificity) for detection of acute LCX injury patterns, with the detection of ST segment elevation in these leads. Later in the acute phase, as myocardial necrosis is evolving and also in the chronic phase, there is an increased amplitude and widening of the R wave in V1, V2 ( as a mirror image of the Q waves of myocardial necrosis in the posterior leads overlying the area of necrosis). In true posterior MI, injury is actually located in portions of the lateral wall of the left ventricle.
Recognition of a true posterior acute MI pattern is important
because it leads to an immediate reperfusion strategy (as in every STEMI). New appearance of these ECG changes, compatible clinical manifestations, or the association with an acute inferior MI are clues to this diagnosis.
In an appropriate clinical setting (acute symptoms raising suspicion of an acute coronary syndrome) coronary occlusion causing transmural myocardial ischemia (an ST elevation myocardial infarction STEMI) is diagnosed by the following ECG findings:
1) In leads V2 -V3, ST segment elevation of 2 mm (0.2 mV) or more at the J point in men, or 1.5 mm (0.15 mV) or more in women in the absence of left ventricular hypertrophy, or
2) in two or more other contiguous chest or limb leads the presence of an ST elevation of 1 mm (0.1 mV) or more. In such patients, emergency reperfusion (primary angioplasty or fibrinolysis) should be performed, unless there is a contraindication.
3) Another diagnostic ECG criterion for a STEMI, if compatible symptoms are also present (i.e., in the appropriate clinical setting) is a new or presumably new LBBB (which may obscure ST elevation analysis). In this case emergency reperfusion is also indicated.
4) Another type of STEMI (in which prompt emergency reperfusion is performed, as for any STEMI) is a true posterior myocardial infarction (MI). True posterior MI in the acute phase presents ST depression in leads V1, V2 (and sometimes also in V3, V4). This is a mirror-image of ST elevation in the posterior leads V7-V9 and is usually caused by an acute infarction in the territoty of a non dominant left circumflex (LCX) coronary artery. In case of suspicion, extending the ECG to left posterior leads V7 -V9 increases sensitivity (also with excellent specificity) for detection of acute LCX injury patterns, with the detection of ST segment elevation in these leads. Later in the acute phase, as myocardial necrosis is evolving and also in the chronic phase, there is an increased amplitude and widening of the R wave in V1, V2 ( as a mirror image of the Q waves of myocardial necrosis in the posterior leads overlying the area of necrosis). In true posterior MI, injury is actually located in portions of the lateral wall of the left ventricle.
Recognition of a true posterior acute MI pattern is important
because it leads to an immediate reperfusion strategy (as in every STEMI). New appearance of these ECG changes, compatible clinical manifestations, or the association with an acute inferior MI are clues to this diagnosis.
With infarction, depolarization (QRS) changes often accompany repolarization (ST-T) abnormalities, if some time has passed and there is necrosis of sufficient myocardial tissue. This can lead to decreased R wave amplitude or abnormal Q waves in the anterior, lateral, or inferior leads as a result of loss of electrical forces in the infarcted area.
The ECG of a male patient, 65 years old, who complained of retrosternal pain since about half an hour, with perspiration. What is: 1) the diagnosis and 2) the proposed treatment?

Answer
1.Acute anterolateral ST elevation myocardial infarction (STEMI). Note the ST segment elevation in the anterior leads V1-V4 and the lateral leads V5,V6 and I and a mirror ST depression in leads III and aVF.
2. Nitrates (if there is no hypotension), aspirin, clopidogrel loading dose (or ticagrelor loading dose),morphine, oxygen administration (particularly if the hemoglobin saturation is below normal) and as soon as possible primary angioplasty (if it can be done within 120 minutes) or thrombolysis if primary angioplasty cannot be performed promptly (at most within 120 minutes). Also heparin (standard or low molecular weight heparin), a beta-blocker (if there is no bradycardia or hypotension), an ACE inhibitor (if there is no hypotension) and a statin.
A man 52 years old, with crushing substernal chest pain. What is the diagnosis and which artery is probably responsible? (the ECG is courtesy of Dr Najeebullah Sajid (facebook group CARDIOCARE)

The rhythm is sinus. There is ST elevation in the lateral leads (I, avL, V5, V6) , thus this is a lateral acute myocardial infarction (STEMI). There is also ST depression in V1 and V2 which can be attributed to an acute posterior myocardial infarction. (If we had placed an ECG lead at the patient's back, facing the posterior wall, this lead would show an ST-segment elevation). ST depression in leads III and avF is due to a mirror image of the ST elevation in the lateral leads. Often in an acute STEMI there is a mirror image of ST depression in leads having a different or opposite direction than the leads which are close to the site of the infarction. Conclusion: An acute ST-elevation myocardial infarction (STEMI) of the lateral and posterior wall (territory of the left circumflex coronary artery-LCX, which is the occluded artery in this case). Emergency reperfusion with a PCI or thrombolysis is required for this patient.
In the chronic phase of a myocardial infarction ST segments may remain elevated suggesting the presence of a dyskinetic or aneurysmatic segment of the left ventricular wall.
Subendocardial ischemia
Subendocardial ischemia
When ischemia is confined primarily to the subendocardium, the ST vector typically shifts toward the inner ventricular layer and the ventricular cavity. Since the current of injury is located only in the inner aspect of the myocardium if we imagine a theoretical lead located into the left ventricle near the ischemic area of the endocardium, this imaginary lead would show ST segment elevation. The leads of the ECG that we obtain in clinical practice are directed toward the epicardial (outer) layer of the heart. Therefore, they will show a mirror image of this current of injury and this is the characteristic ischemic ST-segment depression. The ischemic ST depression is usually horizontal or downsloping and less often slowly upsloping. An ST-segment elevation may be present in lead aVR, which is oriented toward the ventricular cavity.
A male patient, age 53, smoker with a history of low HDL cholesterol ( 33 mg/dl) and a sedentary lifestyle. He did not have a known history of heart disease. He complained of anterior chest pain felt around the sternum. What abnormalities can you see in his ECG and what is the probable diagnosis ?

The rhythm is sinus and the QRS axis is normal. There is a horizontal ST segment depression in leads I, aVL (which also displays T wave inversion), V5 and V6. There is also a subtle ST segment elevation in lead aVR ( because it faces in an opposite direction than the other leads which show ST depression). Although the ST depressions are not very deep in this case (about 1 mm=0.1 mV) they have a characteristic ischemic morphology. The diagnosis is a non ST elevation acute coronary syndrome (NSTEMI or unstable angina depending whether there will be a rise in cardiac troponin or not). The patient should be admitted to the hospital, started on double antiplatelet and anticoagulant treatment (e.g. low molecular weight heparin) plus anti-ischemic treatment (beta-blockers and nitrates if there is no hypotension or other containdications ) and a statin. A coronary angiography is also required preferrably within the first 12-24 hours.
A male patient, age 53, smoker with a history of low HDL cholesterol ( 33 mg/dl) and a sedentary lifestyle. He did not have a known history of heart disease. He complained of anterior chest pain felt around the sternum. What abnormalities can you see in his ECG and what is the probable diagnosis ?

In this case there was a rise and fall in cardiac troponin I, therefore a NSTEMI was confirmed. The coronary angiography showed significant lesions of the circumflex (LCX) and the right coronary artery (RCA) which were both succesfully treated with PCI with placement of drug eluting stents (DES).
Female 70 years old diabetic with dizziness, fatigue, sweating, and vomiting since one hour. On physical examination she has jugular vein distension and hypotension (systolic blood pressure 85 mmHg) What is the cause of hypotension? What should be the treatment and what medication is contraindicated?

Answer:
The ECG shows sinus rhythm (there are normal P waves) and ST elevation in the inferior leads (II, III, avF) and the right precordial leads V3R, V4R . There is also "mirror" ST depression in leads I, avL. Therefore, the diagnosis is an acute inferior myocardial infarcion (MI) with acute right ventricular infarction . This type of infarction is due to an occlusion in the right coronary artery (RCA). In this case, the patient did not have the pain of the infarction, probably due to diabetic neuropathy (typically she should feel pain or pressure on the central area of the chest, sometimes also at the epigastrium). Perspiration (sweating), fatique and nausea are common nonspecific symptoms accompanying an acute MI. Hypotension and jugular vein distention are common clinical findings in a right ventricular (RV) infarction, due to the impairment of the RV contractile function. Right ventricular dysfunction causes both the reduction in cardiac output (leading to hypotension) and the increase in RV diastolic pressure with a consequent increase in right atrial and central venous pressure (leading to jugular venous distention).
In such cases, of an acute inferior MI accompanied by an RV infarction and hypotension, intravenous saline (0.9 % NaCl solution) is administered to raise blood pressure, antiplatelet and anticoagulant treatment (as in every acute MI) and promptly (without delay) urgent reperfusion with angioplasty and stenting. If primary angioplasty within less than 90 minutes is not possible, then thrombolysis is administered. Nitrates are containdicated in an acute RV infarction, even if hypotension is not present.
The negative T wave of ischemic origin is symmetric, usually with an isoelectric or a mildly upsloping ST segment or a horizontally depressed ST segment and appears in leads normally expected to have an upright T wave. It is a common finding, caused either by subendocardial ischemia or by subendocardial necrosis of the myocardium. It may occur as a manifestation of acute coronary syndromes (Non ST elevation myocardial infarction or unstable angina) or in the long term after a Q-wave myocardial infarction. The inverted Q waves often appear after the ischemic episode but they may also appear during the episode with concomitant ST segment depression.
In Non ST elevation acute coronary syndromes (unstable angina or non ST elevation MI-NSTEMI) the ECG often shows negative T waves > 1 mm in leads expected to show an upright T wave, or ST segment depression (usually horizontal or downsloping, less frequently slowly upsloping).
A male patient, 57 years old, smoker with hypercholesterolemia and without any history of cardiac disease, is describing episodes of " squeezing and heaviness" on the central area of the chest, when walking at a usual speed on level ground. Chest discomfort lasts about five minutes and stops when he interrupts walking and rests for a couple of minutes. These symptoms started 15 days ago. Diagnosis? Is there any significant risk on the short-term ? Management?

Answer:
Typical history of recent onset angina at a small effort, . Therefore the history suggests unstable angina, since unstable angina is either angina of recent onset < month at a low workload , or angina with recent increase in symptom severity or frequency (crescendo angina), or angina at rest. The ECG findings are suggestive of a high-risk patient (deep negative, or biphasic T waves in multiple precordial leads). So there is a significant short-term risk of an adverse cardiovascular event (myocardial infarction or death). The ECG pattern cannot be distinguished from the ECG of a patient with a non ST elevation myocardial infarction (NSTEMI). However, the duration of the chest discomfort is consistent with angina (in myocardial infarction chest discomfor lasts usually more than 20 minutes). The distinction between unstable angina and NSTEMI is based on troponin blood levels (the best biomarker for myocardial necrosis), or CKMB, which begin to increase 6-8 hours after the onset of a myocardial infarction. These biomarkers (of myocardial necrosis) do not rise in unstable angina.
Management : Admit to the hospital as a case of probable unstable angina (ECG features of relatively high risk), immediate initiation of antiplatelet (usually aspirin plus loading dose of clopidogrel, or aspirin plus loading dose of one of the newer antiplatelet agents), and anticoagulation treatment (low molecular weight heparin or unfractionated heparin), nitrates, a beta -blocker, initiation of a statin drug and coronary angiography, preferably within the first or second day of hospital stay.
Question 2: On the basis of the ECG picture is it possible to suspect which should be the culprit vessel?
Answer:
This pattern of diffuse prominent T wave inversion in the precordial leads is usually suggestive of a severe stenosis of the proximal left anterior descending (LAD) branch of the left coronary artery.
Indeed, the patient's coronary angiography showed this type of lesion. He was treated with angioplasty and placement of a coronary stent (percutaneous coronary intervention -PCI).
---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
A man, 55 years old, with a history of hypercholesterolemia and no other cardiac history. In the last four days, he had several episodes of constrictive retrosternal pain, of a few minutes duration, occurring with physical activity of low intensity. Physical examination was without remarkable findings. His resting ECG (he had no discomfort during the ECG) is given below. What are the ECG findings? In this case, what is of greater diagnostic importance, the patient's history or the ECG findings? What is the proposed further diagnostic and therapeutic strategy?

Sinus rhythm, normal QRS frontal plane axis, small negative T wave in aVL, V4, V5 and flattened T wave in lead I. These ECG findings can raise a suspicion of underlying coronary artery disease but they are not specific. In this case, the history is more important for the diagnosis, and it is suggestive of angina on small effort of a very recent onset. Therefore, the history suggests unstable angina. In this context, ECG findings of inverted T waves enhance these diagnostic thoughts. The patient was admitted to the hospital, treatment for unstable angina was initiated, with dual antiplatelet drug treatment, low molecular weight heparin, a nitroglycerin patch, a beta-blocker, a statin and a decision to proceed with coronary angiography (within 24-48 hours). There was no rise in troponin, so it was not a NSTEMI, but unstable angina. Coronary angiography showed a severe stenosis (90% in the mid-right coronary artery), which was treated by angioplasty with stenting. Dual antiplatelet therapy was given for 12 months (together with pantoprazole for gastric protection), and then antiplatelet therapy was continued with aspirin only, while the administration of a statin and a low dose of a beta-blocker was also continued.
Note: The ECG findings (small inverted T waves) resolved promptly after percutaneous coronary intervention (PCI). An important observation is that the leads with T wave inversion do not accurately identify the coronary artery involved (as opposed to the finding of ST-segment elevation). An exception is Wellens syndrome in which deep symmetric negative or biphasic T waves are present in the precordial leads (usually from V2 to V4 but quite often also in V5 and V6), without Q waves or ST-segment elevation ≥1 mm in these leads. This syndrome is associated with a severe proximal stenosis of the left anterior descending coronary artery (LAD).
Acute pericarditis (due to an acute inflammation of the pericardium) typically is characterized by diffuse ST segment elevation, usually in most of the chest leads and also in leads I, aVL, II, and aVF. Reciprocal ST segment depression is often present in lead aVR. The diffuse nature of the ST segment elevation in acute pericarditis is an important difference from the pattern seen in acute ST elevation myocardial infarction (STEMI). (In STEMI the ST segment elevation is not diffuse. It is observed in leads corresponding to a coronary artery territory and there are often reciprocal ST depressions in leads located away from the area of the infarction). Another important characteristic in acute pericarditis is the frequent presence of PR segment elevation in aVR, with reciprocal PR segment depression in many other leads, caused by the coexistence of an atrial current of injury. In acute pericarditis abnormal Q waves do not appear and the ST segment elevation may be followed by T wave inversion after a variable period of time.
A male patient, 57 years old, smoker with hypercholesterolemia and without any history of cardiac disease, is describing episodes of " squeezing and heaviness" on the central area of the chest, when walking at a usual speed on level ground. Chest discomfort lasts about five minutes and stops when he interrupts walking and rests for a couple of minutes. These symptoms started 15 days ago. Diagnosis? Is there any significant risk on the short-term ? Management?

Answer:
Typical history of recent onset angina at a small effort, . Therefore the history suggests unstable angina, since unstable angina is either angina of recent onset < month at a low workload , or angina with recent increase in symptom severity or frequency (crescendo angina), or angina at rest. The ECG findings are suggestive of a high-risk patient (deep negative, or biphasic T waves in multiple precordial leads). So there is a significant short-term risk of an adverse cardiovascular event (myocardial infarction or death). The ECG pattern cannot be distinguished from the ECG of a patient with a non ST elevation myocardial infarction (NSTEMI). However, the duration of the chest discomfort is consistent with angina (in myocardial infarction chest discomfor lasts usually more than 20 minutes). The distinction between unstable angina and NSTEMI is based on troponin blood levels (the best biomarker for myocardial necrosis), or CKMB, which begin to increase 6-8 hours after the onset of a myocardial infarction. These biomarkers (of myocardial necrosis) do not rise in unstable angina.
Management : Admit to the hospital as a case of probable unstable angina (ECG features of relatively high risk), immediate initiation of antiplatelet (usually aspirin plus loading dose of clopidogrel, or aspirin plus loading dose of one of the newer antiplatelet agents), and anticoagulation treatment (low molecular weight heparin or unfractionated heparin), nitrates, a beta -blocker, initiation of a statin drug and coronary angiography, preferably within the first or second day of hospital stay.
Question 2: On the basis of the ECG picture is it possible to suspect which should be the culprit vessel?
Answer:
This pattern of diffuse prominent T wave inversion in the precordial leads is usually suggestive of a severe stenosis of the proximal left anterior descending (LAD) branch of the left coronary artery.
Indeed, the patient's coronary angiography showed this type of lesion. He was treated with angioplasty and placement of a coronary stent (percutaneous coronary intervention -PCI).
---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
A man, 55 years old, with a history of hypercholesterolemia and no other cardiac history. In the last four days, he had several episodes of constrictive retrosternal pain, of a few minutes duration, occurring with physical activity of low intensity. Physical examination was without remarkable findings. His resting ECG (he had no discomfort during the ECG) is given below. What are the ECG findings? In this case, what is of greater diagnostic importance, the patient's history or the ECG findings? What is the proposed further diagnostic and therapeutic strategy?

Sinus rhythm, normal QRS frontal plane axis, small negative T wave in aVL, V4, V5 and flattened T wave in lead I. These ECG findings can raise a suspicion of underlying coronary artery disease but they are not specific. In this case, the history is more important for the diagnosis, and it is suggestive of angina on small effort of a very recent onset. Therefore, the history suggests unstable angina. In this context, ECG findings of inverted T waves enhance these diagnostic thoughts. The patient was admitted to the hospital, treatment for unstable angina was initiated, with dual antiplatelet drug treatment, low molecular weight heparin, a nitroglycerin patch, a beta-blocker, a statin and a decision to proceed with coronary angiography (within 24-48 hours). There was no rise in troponin, so it was not a NSTEMI, but unstable angina. Coronary angiography showed a severe stenosis (90% in the mid-right coronary artery), which was treated by angioplasty with stenting. Dual antiplatelet therapy was given for 12 months (together with pantoprazole for gastric protection), and then antiplatelet therapy was continued with aspirin only, while the administration of a statin and a low dose of a beta-blocker was also continued.
Note: The ECG findings (small inverted T waves) resolved promptly after percutaneous coronary intervention (PCI). An important observation is that the leads with T wave inversion do not accurately identify the coronary artery involved (as opposed to the finding of ST-segment elevation). An exception is Wellens syndrome in which deep symmetric negative or biphasic T waves are present in the precordial leads (usually from V2 to V4 but quite often also in V5 and V6), without Q waves or ST-segment elevation ≥1 mm in these leads. This syndrome is associated with a severe proximal stenosis of the left anterior descending coronary artery (LAD).
Acute pericarditis (due to an acute inflammation of the pericardium) typically is characterized by diffuse ST segment elevation, usually in most of the chest leads and also in leads I, aVL, II, and aVF. Reciprocal ST segment depression is often present in lead aVR. The diffuse nature of the ST segment elevation in acute pericarditis is an important difference from the pattern seen in acute ST elevation myocardial infarction (STEMI). (In STEMI the ST segment elevation is not diffuse. It is observed in leads corresponding to a coronary artery territory and there are often reciprocal ST depressions in leads located away from the area of the infarction). Another important characteristic in acute pericarditis is the frequent presence of PR segment elevation in aVR, with reciprocal PR segment depression in many other leads, caused by the coexistence of an atrial current of injury. In acute pericarditis abnormal Q waves do not appear and the ST segment elevation may be followed by T wave inversion after a variable period of time.
A woman 60 years old presenting with pain on the substernal area and the precordium since 12 hours. The pain increases when lying flat and with deep inspiration. What are the ECG findings and what is the proposed diagnostic testing and probable treatment ?
 |
| ECG -cardiology case |
Answer
The ECG shows sinus rhythm and normal QRS frontal axis. There is PR segment depression (note that the PR segment is at a lower level than the TP segment) in many leads (II, aVF, V2-V6) and PR segment elevation in avR. There is also a mild ST segment elevation (concave upward) in some leads (V2-V5, II). These ECG findings and the characteristics of the pain raise a suspicion of acute pericarditis, although the ECG is not completely typical (usually in acute pericarditis the concave upward ST segment elevation is more diffuse-present in more leads- and more prominent, than in this ECG). However the ECG , as mentioned above, shows some features suggestive of acute pericarditis. Testing should include the usual general blood tests plus c-reactive protein (CRP) and echocardiography. In this case, blood tests showed an elevated leukocyte count (13000/ μL) and moderately elevated CRP. Cardiac troponin test was negative. Echocardiography in this case showed a small pericardial effusion. Treatment of acute pericarditis should be with non steroidal anti-inflammatory drugs (NSAIDs: usually aspirin, ibuprofen, indomethacin, or naproxen) at least for about 2 weeks usually in combination with a drug protective for the stomach (e.g. omeprazol, lansoprazol, pantoprazol, or ranitidine). A full-dose NSAID should be maintained until normalization of the C-reactive protein (CRP) followed by gradual tapering of the drug for another 1-2 weeks to prevent early reoccurrence. In more severe cases of acute pericarditis (e.g. with severe pain showing a delayed response to treatment with a NSAID, or with a moderate to large pericardial effusion), or in reccurent pericarditis concomitant administration of colchicine (combined with the administration of NSAIDS) can improve treatment effectiveness and reduce the posibility of further recurrences. (See chapter "Acute pericarditis -pericardial effusion").
The QT interval, is measured from the onset of the QRS complex to the end of the T wave. The QT interval is generally measured in leads II, V5 and V6 and reported as the longest interval among the three. If the QT interval cannot be accurately measured in these leads, other leads can be used. The QT interval increases in slow heart rates and decreases in fast heart rates, so it must be corrected for the heart rate, in order to assess if it is normal, prolonged or decreased.
Bazett’s formula defines a corrected QT interval (QTc):QTc=QT/√RR
Bazett’s formula works well at heart rates within the normal range but overcorrects at high rates (so at high rates it gives a QTc relatively greater than real) and undercorrects at low rates (estimating again a QTc relatively greater than real). The upper limit of a normal QTc is in men 0.45 second (450 msec) and in women 0.46 second (460 msec) . Patients with a congenital or acquired prolonged QTc, especially if it is markedly prolonged (480 msec or more) may be at risk for torsades de pointes ventricular tachycardia.A short QTc interval (<390 msec) is rare, but it also carries an increased risk of malignant ventricular arrhythmias.
Hypokalemia (reduced potasium concentration in the blood) causes prolongation of the QTc ( for the ECG features of hypokalemia see below).
Left ventricular hypertrophy (LVH)
The most characteristic finding is increased amplitude of the R waves in leads facing the left ventricle ( I, aVL, V5, and V6), which are taller than normal, and S waves in leads V1 and V2, overlying the opposite side of the heart, are deeper than normal.
In leads with tall R waves usually the ST segment is depressed (typically, it slopes downward from a depressed J point) and the T wave is inverted and asymmetric. In some patients in leads with a tall R wave the ST segment may be normal or somewhat elevated. These repolarization changes (ST depression and T wave inversion) in patients with left ventricular hypertrophy (LVH) usually occur in
patients with QRS changes, but they may also appear alone. There are numerous criteria for diagnosing LVH and they are more reliable in people over 40 years of age (because in some normal young persons there is an increased amplitude of the QRS ). Some useful criteria are: The Sokolow-Lyon voltage criteria :
The sum of the S wave in V1 or V2 and the R-wave in V5 or V6 > 35 mm (3.5 mV). The R wave in aVL ≥ 12 mm (1.2 mV).
The Romhilt-Estes point score system (probable LVH=4 points/ definite LVH=5 points)
Any limb lead R wave or S wave > 20 mm , or SV1 or SV2 ≥ 30 mm , or RV5 to RV6 ≥ 30 mm (3 points)
ST-T wave abnormality in a patient with no digitalis therapy (3 points)
ST-T wave abnormality in a patient receiving digitalis therapy (1 point)
Left atrial abnormality (3 points)
Left axis deviation ≥−30 degrees (2 points)
QRS duration ≥90 msec (1 point)
Intrinsicoid deflection (the time interval from the onset of the QRS to the peak of the R wave) in V5 or V6 ≥50 msec (1 point).
ECG criteria for LVH, have a high specificity (when they are present, there is a high probability that LVH is actually present, (this corresponds to a low proportion of false positive findings), but a low sensitivity (there is a relatively high proportion of false negative findings : people that have LVH as shown with echocardiography, but do not have the ECG criteria.)
LVH usually occurs with left ventricular pressure overload (work of the left ventricle under conditions of increased systolic ventricular pressure, for example in arterial hypertension, or in aortic valve stenosis). Hypertrophic cardiomyopathy is another cause of left ventricular hypertrophy, often asymmetric.
The ECG has a low sensitivity (about 15 %) , but a high specificity (about 80%) for the diagnosis of LVH. So it cannot exclude LVH (many people with LVH can have a normal ECG, due to the low specificity), but if it shows features of LVH, there is a high probability that more accurate tests (usually echocardiogaphy) will confirm that the patient indeed has LVH. The latter is a feature of high specificity (low number of false positive results).
Right Ventricular Hypertrophy (RVH ) occurs with right ventricular pressure overload (due to pulmonary valve stenosis, which is usually a congenital condition, or pulmonary hypertension)
Typically there is a right axis deviation and an increased R-wave amplitude in the right precordial leads (R wave > S wave in lead V1).
Common diagnostic criteria for RVH are the following:
The QRS in lead V1: an R ≥ 7 mm (0.7 mV), an R/S >1 with an R > 5 mm, or a QR or qR pattern.
The increased R in V1 is due to this lead's position in proximity of the right ventricle, recording its increased electrical forces in RVH.
Criteria regarding the QRS in V5 or V6 are based on the fact that these leads are oriented towards the left ventricle and away from the right ventricle. So, the increased right ventricular electrical activity causes a partial cancellation of left ventricular electrical forces in these leads ( low R wave) and also the appearance of a more prominent S wave. So in leads V5 or V6 common criteria for RVH include R/S <1 (S>R), or an S wave> 7 mm.
Other criteria of RVH :
Right axis deviation (>90 degrees)
S1Q3 pattern (this means the presence of a large S wave in lead I, either a RS or rS pattern, and an abnormal Q wave in lead III).
S1S2S3 pattern (large S waves in leads I, II and III)
P pulmonale (ECG pattern of a right atrial abnormality-see section on P wave).
Woman, age 27 with effort dyspnea and fatigue. These symptoms worsened progressively in the last 6 months. Physical examination showed blood pressure 110/80 mmHg, jugular venous distention with increased height of visible jugular venous pulsations , with prominent a and v waves. Auscultation revealed an increased intensity of the second heart sound parasternally at the second and third left intercostal space and no audible murmurs. Auscultation of the lungs was normal. The ECG is given below. What are the ECG findings and what is the differential diagnosis?

Answer
Physical examination showed signs compatible with right ventricular (RV) dysfunction: Dilated external jugular veins and increased height of visible pulsations of the internal jugular veins, which indicate an elevated central venous pressure/ prominent a-wave of the jugular venous pulse indicative of an elevated RV end diastolic pressure/ prominent v wave indicative of tricuspid regurgitation (which in many cases can be severe, without an audible holosystolic murmur). The increased intensity of the second heart sound (S2) parasternally at the second left intercostal space, since this is the area of the pulmonic valve, is due to an augmented pulmonic component of the second heart sound (P2) and is suggestive of pulmonary hypertension.
The ECG shows sinus rhythm, P waves have an increased amplitude (indicative of right atrial enlargement) and QRS frontal plain axis shows right deviation, In the right precordial leads R waves have an increased amplitude and in lead V1 there is a qR pattern. There are also inverted Τ waves in the precordial leads and in the left precordial leads V5 and V6 an increased amplitude of the S wave is noted. This ECG pattern indicates right ventricular hypertrophy. The ECG picture, combined with the symptoms and physical signs is suggestive of pulmonary hypertension. Another cause of RV hypertrophy is pulmonic stenosis (PS), but in this case the physical findings do not support this diagnosis ( in PS there is a systolic ejection murmur heard over the pulmonic area and a diminished intensity of P2). Thus the differential diagnosis in this case includes causes of pulmonary hypertension. Echocardiography is absolutely necessary and other diagnostic tests will follow depending on the findings, in order to reach an etiologic diagnosis. (Note :Tricuspid regurgitation is often secondary, due to RV enlargement, which causes displacement of the papillary muscles and dilatation of the tricuspid annulus). In this case the final diagnosis was idiopathic pulmonary hypertension (a rare cause of pulmonary arterial hypertension).
-----------------------------------------------------------------
Male patient 69 years old with a history of hypertension and hypercholesterolemia. The patient denies any anginal symptoms or any other symptoms on ordinary physical activity. Physical examination revealed arrhythmia, normal heart sounds without a cardiac murmur and blood pressure 170/80 mmHg. What abnormalities can you see in his ECG, what are your diagnostic thoughts and what is the proposed further diagnostic evaluation and treatment?
 quiz-cardiology book")
The rhythm is atrial fibrillation (absent P waves, fine fibrillatory waves and variable RR intervals) with a slow ventricular rate. QRS frontal plane axis is normal. There is a deep S wave in lead V2, tall R wave in leads V5 ( almost 30 mm), a positive Sokolow index ( RV5+SV1 > 35 mm) and abnormal negative T waves in leads I, avL, V4-V6 (the T wave is biphasic in lead V3). The voltage criteria and the T wave abnormalities are consistent with a diagnosis of left ventricular hypertrophy due to hypertensive heart disease. Atrial fibrillation is also common in hypertensive heart disease. Although the diagnosis of secondary T wave changes due to left ventricular hypertrophy is the most probable explanation for the inverted T waves in this ECG, they could also be due to coronary artery disease. Further diagnostic testing was with echocardiography, which revealed concentric left ventricular (LV) hypertrophy (diastolic wall thickness of the interventricular septum and the posterior wall of 13 mm-upper limit of normal 11mm) with normal LV dimensions and normal systolic function. The left atrium was enlarged and there was a moderate mitral regurgitation (functional due to a dilated mitral annulus). Myocardial perfusion scintigraphy (cardiac SPECT scan) was also undertaken to assess for myocardial ischemic disease. The SPECT was almost normal, without perfusion defects of a significant extent or severity. Hypertension was controlled (with an ACE inhibitor in combination with thiazide diuretic plus a calcium channel blocker) and oral anticoagulation was started, because of atrial fibrillation with a CHA2DS2-VASc score of 2. When this score in patients with atrial fibrillation (permanent, persistent or paroxysmal) is 1 or more in men and 2 or more in women, chronic thromboembolic prophylaxis with an oral anticoagulant is indicated. (see the chapter on tachyarrhythmias Tachyarrhythmias-supraventricular and ventricular tachycardias) Choices for anticoagulation include one of the newer anticoagulants (non vitamin K antagonist oral anticoagulants-NOACS, e.g dabigatran, apixaban, rivaroxaban or endoxaban) or a vitamin K antagonist (such as warfarin or acenocoumarol) with a target INR 2-3.
Hyperkalemia
The earliest effect is peaking (tenting) and narrowing of the T wave, which becomes tall. With progressive hyperkalemia P wave amplitude decreases and QRS begins to widen. PR interval prolongation can occur (and sometimes second or third degree atioventricular block). Complete loss of P waves may occur, associated with a junctional escape rhythm or so-called sinoventricular rhythm. Moderate to severe hyperkalemia occasionally induces elevation of the ST segment in the right precordial leads (V1 and V2).
Chronic renal failure The ECG triad of peaked T waves (from hyperkalemia), QT prolongation (from hypocalcemia), and left ventricular hypertrophy (from hypertension) is suggestive of chronic renal failure.
Hypokalemia, causes hyperpolarization of myocardial cell membranes and increased action potential duration. The ECG
manifestations include ST depression with flattened T waves and increased U wave prominence (U waves become enlarged). The U waves can exceed in amplitude the T waves. The T waves can be flattened or negative. The QT interval is prolonged. Because the T waves and U waves often merge, in some cases the QT interval cannot be accurately measured.
Describe the findings in this ECG

Rhythm sinus, QRS axis normal, widespread ST depression and T wave inversion and prominent (large) U waves (here especially in the leads II, aVF, V2-V5). These are findings suggestive of hypokalemia. Serum potasium was 2 mEq/L in this patient (Normal K levels 3.5-5.5 mEq/L).
The pediatric ECG
The normal resting heart rate varies with age. The average resting heart rate increases from birth to 1 month of age and subsequently decreases.The increase in heart rate in the first month of life is related to the activity of the autonomic nervous system, but the subsequent decrease of heart rate is primarily related to age-dependent changes in the intrinsic sinus node activity.
Here are some normal limits (simplified ) in beats per minute (bpm) :
first week of life 90-160 (mean 124) bpm
-hyperkalemia-cardiology book") |
| Lead V5 of a patient with hyperkalemia. Note the T wave which becomes tall and narrow. |
Chronic renal failure The ECG triad of peaked T waves (from hyperkalemia), QT prolongation (from hypocalcemia), and left ventricular hypertrophy (from hypertension) is suggestive of chronic renal failure.
Hypokalemia, causes hyperpolarization of myocardial cell membranes and increased action potential duration. The ECG
manifestations include ST depression with flattened T waves and increased U wave prominence (U waves become enlarged). The U waves can exceed in amplitude the T waves. The T waves can be flattened or negative. The QT interval is prolonged. Because the T waves and U waves often merge, in some cases the QT interval cannot be accurately measured.
Describe the findings in this ECG

Rhythm sinus, QRS axis normal, widespread ST depression and T wave inversion and prominent (large) U waves (here especially in the leads II, aVF, V2-V5). These are findings suggestive of hypokalemia. Serum potasium was 2 mEq/L in this patient (Normal K levels 3.5-5.5 mEq/L).
The pediatric ECG
The normal resting heart rate varies with age. The average resting heart rate increases from birth to 1 month of age and subsequently decreases.The increase in heart rate in the first month of life is related to the activity of the autonomic nervous system, but the subsequent decrease of heart rate is primarily related to age-dependent changes in the intrinsic sinus node activity.
Here are some normal limits (simplified ) in beats per minute (bpm) :
first week of life 90-160 (mean 124) bpm
7 days –6 months 105–180 (mean 145) bpm
6-12 months 105–170 (mean 130) bpm
Years 1–3 90–150 (mean 120) bpm
Years 3–5 70–135 (mean 105) bpm
Years 5–12 60–130 (mean 95) bpm
Years 12-16 60–120 (mean 80) bpm
The morphology of a normal ECG varies with age. In young children the electrical forces of the right ventricle are more evident than in adults. A right deviation of the QRS frontal axis is normal through the first year of life.
Three patterns can be distinguished, through the morphology of the QRS complex (ventricular depolarization) and the T wave (ventricular repolarization):
The neonatal pattern ECG is typical in the first month of life.
In a normal child, this ECG pattern changes after the first month and takes on the characteristics of the infant pattern, which can last up to the age of three.
After the age of 3 years the ECG changes again, gradually taking the characteristics of the adult pattern.
Normally, the ECG pattern is in concordance with the age of the patient.
An ECG pattern different from what would be expected according to the patient’s age, (for example a neonatal pattern after the first month of life), should lead to the suspision of a pathological reason.
Important note : The term “infant”, referring to a child in the first year of life, is not equivalent to the term “infant ECG pattern”, which can last until the age of about 3 years.
The neonate ECG pattern, normally shows a prevalent electrical activity of the right ventricle.
This is a result of the hemodynamic condition of a fetus. After the 31st week of gestation until term, the right ventricle of the fetus gains myocardial mass because it pumps against the high resistance of the small muscular pulmonary arteries. The left ventricle pumps against the low resistance of the placenta’s blood vessels. At birth the mass of the right and left ventricles have a ratio of 1 :1.3 . This ratio is quite different from the adult person, where left ventricular mass is much larger than right ventricular mass.
Lead V1 is the precordial lead facing the right ventricle. Thus, in lead V1 the depolarizing electrical activity of the right ventricle is represented by the R wave (the positive deflection) and the depolarizing electrical activity of the left ventricle is represented by the S wave.
Lead V6 faces the left ventricle. Thus in this lead, the R wave (positive deflection) corresponds to the depolarizing electrical activity of the left ventricle and the S wave (negative deflection) represents the depolarization of the right ventricle.
Since the electrical activity of the right ventricle prevails in the first mont of age, the neonate ECG pattern has the following features: In lead V1 the R wave is dominant (R/S > 1) and in lead V6 the dominant wave is S (R/S < 1).
In V1 the R wave can be exclusive (without an S), but in that case, its voltage should be less than 13 mm (1.3 mV) in the first week of life and less than 10 mm (1 mV) afterwards. If an S wave is also present in V1, then the R/S ratio: is from 1 to 7, R wave < 25 mm and S wave < 20 mm.
In lead V6 R< S and also S wave < 10 mm.
With regards to the morphology of the T wave, in the first week of life, in lead V1 T wave can be positive or negative and T wave in lead V6 usually is positive (but a flat or negative T wave in V6 in the first week of life is considered at the limits of normal, i.e. a normal variant ).
After the first week of life the neonatal pattern is characterized by the following : T wave in leads V1 and V2 must be negative and in V6 it must be positive.
A positive T wave in V1 after the first week of life should be regarded with suspicion and investigated because it can indicate right ventricular hypertrophy, elevated systolic pressure in the right ventricle and /or elevated pulmonary vascular resistance (PVR). These findings can be caused by congenital heart disease.
Within the first few hours after birth hemodynamic changes begin, which continue over the next months and years and form the basis of the changes in the ECG. After birth and as the child grows, there is a gradual fall in pulmonary vascular resistance (PVR) which causes a gradual reduction in right ventricular systolic pressure. Consequently, right ventricular mass (in comparison to left ventricular mass) and right ventricular electrical forces gradually decrease, as the circulation of the growing child matures.
The left ventricle, after birth and as the child grows, follows the opposite course. After birth it ceases to pump against the low resistance of the blood vessels in the placenta and begins pumping against the high resistance of the peripheral blood vessels. This causes a rise in left ventricular systolic pressure and a gradual rise in left ventricular mass, and left ventricular electrical force. These changes continue throughout the first years of life, with the right ventricle (having to pump against a smaller resistance) growing more slowly than the left ventricle and this reflects on the evolution of the ventricular electrical forces in the ECG.
The “infant ECG pattern” is characterized by balanced ventricular electrical forces. This is the normal ECG pattern found after the first month of life up to 2-3 years. After the first month of life the electrical forces of the ventricles are balanced, therefore, the infant ECG pattern shows equal electrical weight of the two ventricles.
In lead V1 the R wave will still be dominant ( R/S > 1) but the normal R wave voltage is < 20 mm (2 mV). Sometimes in V1 the R wave may be exclusive. In that case, to be normal, its voltage should be < 10 mm (1 mV). An exclusive R in V1 should never be present after the first year of life.
In V6 the R wave will be dominant over the S wave (R/S > 1). The normal R in V6 should be < 25 mm (2.5 mV) and the S wave <10 mm (1 mV). As a general rule, R waves are usually prominent in the right precordial leads in neonates and infants but gradually decrease in amplitude with age.
A unique characteristic of the infant pattern, is that potentially a narrow Q wave ≤ 10 mm can be present in the inferior leads (II, III, aVF) and/or lead V6.
In infants, Q waves are usually absent in leads I and aVL, and if they are present, they are often suggestive of cardiac pathology. A deep (.3 mm) and broad (.30 ms) Q wave in leads I and aVL, especially when Q waves are absent in the inferior leads, may suggest the diagnosis of anomalous origin of the left coronary artery from the pulmonary artery. The presence of Q waves in the right precordial leads in infants and children is always pathologic. They are commonly associated with right ventricular hypertrophy.
Deep Q waves in the left lateral precordial leads (V5,V6) are often present in left ventricular hypertrophy of many etiologies. Q waves ≥ .3mm in depth or ≥ . .40 ms in duration, in .two or more leads other than V1,V2, or III, raise a suspicion of familial hypertrophic cardiomyopathy (this finding has low sensitivity, but high specificity).
Regarding repolarization, in the infant ECG pattern the T wave in leads V1-V3 is normally negative and this finding can be present as late, as the age of 8-10 years (or sometimes even persist in an adult as a normal variant).
Upright T waves in the right precordial leads prior to age 7 years can raise a suspicion of right ventricular hypertrophy.
The infant ECG pattern, as well as the ECG pattern later in life, is characterized by a T wave in lead V6, which is normally positive.
6-12 months 105–170 (mean 130) bpm
Years 1–3 90–150 (mean 120) bpm
Years 3–5 70–135 (mean 105) bpm
Years 5–12 60–130 (mean 95) bpm
Years 12-16 60–120 (mean 80) bpm
The morphology of a normal ECG varies with age. In young children the electrical forces of the right ventricle are more evident than in adults. A right deviation of the QRS frontal axis is normal through the first year of life.
Three patterns can be distinguished, through the morphology of the QRS complex (ventricular depolarization) and the T wave (ventricular repolarization):
The neonatal pattern ECG is typical in the first month of life.
In a normal child, this ECG pattern changes after the first month and takes on the characteristics of the infant pattern, which can last up to the age of three.
After the age of 3 years the ECG changes again, gradually taking the characteristics of the adult pattern.
Normally, the ECG pattern is in concordance with the age of the patient.
An ECG pattern different from what would be expected according to the patient’s age, (for example a neonatal pattern after the first month of life), should lead to the suspision of a pathological reason.
Important note : The term “infant”, referring to a child in the first year of life, is not equivalent to the term “infant ECG pattern”, which can last until the age of about 3 years.
The neonate ECG pattern, normally shows a prevalent electrical activity of the right ventricle.
This is a result of the hemodynamic condition of a fetus. After the 31st week of gestation until term, the right ventricle of the fetus gains myocardial mass because it pumps against the high resistance of the small muscular pulmonary arteries. The left ventricle pumps against the low resistance of the placenta’s blood vessels. At birth the mass of the right and left ventricles have a ratio of 1 :1.3 . This ratio is quite different from the adult person, where left ventricular mass is much larger than right ventricular mass.
Lead V1 is the precordial lead facing the right ventricle. Thus, in lead V1 the depolarizing electrical activity of the right ventricle is represented by the R wave (the positive deflection) and the depolarizing electrical activity of the left ventricle is represented by the S wave.
Lead V6 faces the left ventricle. Thus in this lead, the R wave (positive deflection) corresponds to the depolarizing electrical activity of the left ventricle and the S wave (negative deflection) represents the depolarization of the right ventricle.
Since the electrical activity of the right ventricle prevails in the first mont of age, the neonate ECG pattern has the following features: In lead V1 the R wave is dominant (R/S > 1) and in lead V6 the dominant wave is S (R/S < 1).
In V1 the R wave can be exclusive (without an S), but in that case, its voltage should be less than 13 mm (1.3 mV) in the first week of life and less than 10 mm (1 mV) afterwards. If an S wave is also present in V1, then the R/S ratio: is from 1 to 7, R wave < 25 mm and S wave < 20 mm.
In lead V6 R< S and also S wave < 10 mm.
With regards to the morphology of the T wave, in the first week of life, in lead V1 T wave can be positive or negative and T wave in lead V6 usually is positive (but a flat or negative T wave in V6 in the first week of life is considered at the limits of normal, i.e. a normal variant ).
After the first week of life the neonatal pattern is characterized by the following : T wave in leads V1 and V2 must be negative and in V6 it must be positive.
A positive T wave in V1 after the first week of life should be regarded with suspicion and investigated because it can indicate right ventricular hypertrophy, elevated systolic pressure in the right ventricle and /or elevated pulmonary vascular resistance (PVR). These findings can be caused by congenital heart disease.
Within the first few hours after birth hemodynamic changes begin, which continue over the next months and years and form the basis of the changes in the ECG. After birth and as the child grows, there is a gradual fall in pulmonary vascular resistance (PVR) which causes a gradual reduction in right ventricular systolic pressure. Consequently, right ventricular mass (in comparison to left ventricular mass) and right ventricular electrical forces gradually decrease, as the circulation of the growing child matures.
The left ventricle, after birth and as the child grows, follows the opposite course. After birth it ceases to pump against the low resistance of the blood vessels in the placenta and begins pumping against the high resistance of the peripheral blood vessels. This causes a rise in left ventricular systolic pressure and a gradual rise in left ventricular mass, and left ventricular electrical force. These changes continue throughout the first years of life, with the right ventricle (having to pump against a smaller resistance) growing more slowly than the left ventricle and this reflects on the evolution of the ventricular electrical forces in the ECG.
The “infant ECG pattern” is characterized by balanced ventricular electrical forces. This is the normal ECG pattern found after the first month of life up to 2-3 years. After the first month of life the electrical forces of the ventricles are balanced, therefore, the infant ECG pattern shows equal electrical weight of the two ventricles.
In lead V1 the R wave will still be dominant ( R/S > 1) but the normal R wave voltage is < 20 mm (2 mV). Sometimes in V1 the R wave may be exclusive. In that case, to be normal, its voltage should be < 10 mm (1 mV). An exclusive R in V1 should never be present after the first year of life.
In V6 the R wave will be dominant over the S wave (R/S > 1). The normal R in V6 should be < 25 mm (2.5 mV) and the S wave <10 mm (1 mV). As a general rule, R waves are usually prominent in the right precordial leads in neonates and infants but gradually decrease in amplitude with age.
A unique characteristic of the infant pattern, is that potentially a narrow Q wave ≤ 10 mm can be present in the inferior leads (II, III, aVF) and/or lead V6.
In infants, Q waves are usually absent in leads I and aVL, and if they are present, they are often suggestive of cardiac pathology. A deep (.3 mm) and broad (.30 ms) Q wave in leads I and aVL, especially when Q waves are absent in the inferior leads, may suggest the diagnosis of anomalous origin of the left coronary artery from the pulmonary artery. The presence of Q waves in the right precordial leads in infants and children is always pathologic. They are commonly associated with right ventricular hypertrophy.
Deep Q waves in the left lateral precordial leads (V5,V6) are often present in left ventricular hypertrophy of many etiologies. Q waves ≥ .3mm in depth or ≥ . .40 ms in duration, in .two or more leads other than V1,V2, or III, raise a suspicion of familial hypertrophic cardiomyopathy (this finding has low sensitivity, but high specificity).
Regarding repolarization, in the infant ECG pattern the T wave in leads V1-V3 is normally negative and this finding can be present as late, as the age of 8-10 years (or sometimes even persist in an adult as a normal variant).
Upright T waves in the right precordial leads prior to age 7 years can raise a suspicion of right ventricular hypertrophy.
The infant ECG pattern, as well as the ECG pattern later in life, is characterized by a T wave in lead V6, which is normally positive.
Is this ECG of a 1 year old child, normal ?

Answer
Normal. For details see text.
The adult ECG pattern (in childhood)
The adult ECG pattern usually appears in children older than 2 years and is characterized by prevalent electrical activity in the left ventricle, which is dominant over the electrical activity of the right ventricle. This ECG pattern is the norm after 2–3 years of life.
In V1 the S wave will dominate (R/S <1) . Although the R wave in V1 tends to be taller in a child than in an adult, after the age of 3 years, it will usually be smaller than the S wave. The normal S in V1 must be < 25 mm.
In V6 the R wave is dominant ( R/S > 1) Normally in V6, R wave < 25 mm and S wave < 5 mm.
[In case of an increased amplitude (exceeding normal limits) of the R or S wave in lead V1, or in leads V5, or V6 – or in case of an abnormal R/S relation in these leads- in comparison with the expected findings according to age, or in case of an ECG pattern different from that expected with respect to age : Then there will be a suspicion of hypertrophy or dilatation of one of the two ventricles. In such cases echocardiography is the next step, to search for (or exclude) any abnormality.]
The T wave in lead V6 is positive and in leads V1-V3 is negative up until adolescence (in girls, even later). A positive T wave in leads V2 and V3 may be present in childhood, as a normal variant.
ECG of a six year old girl. Is it normal ?
 |
| Electrocardiogram (ECG) child
Answer
Νormal ECG : Sinus rhythm, normal QRS axis, QT interval within normal limits. The R wave in V1 is somewhat taller than what would be expected in the ECG of an adult person, but this a usual finding in children. It is smaller than the S wave, so it is normal. In leads V5 and V6 R/S is >1 which is normal. The negative T waves in the right precordial leads are normal for a child. Moreover, in order to characterize this ECG as normal the T wave must be positive in leads V5, V6 (it is in this case). For more details see text .
|
QRS axis
As would be expected from the right ventricular dominance of the term infant, the frontal plane QRS axis in term infants is usually directed rightward and inferiorly. Healthy preterm infants may have a more leftward QRS axis.
In term infants, the rightward QRS axis usually within the first year of life changes to a more adult (less rightward) pattern.Thus, the initial right deviation of the QRS frontal axis progressively reduces and turns toward normal.
In the 1st month of life the QRS axis is normally over +120° (right deviated). In the first week of life it can be up to +180°/+210° . Except for individual variation, the QRS frontal axis generally after the age of 6 months should be under +120° , and after the age of 1 year, it should be under +100° .
While in adults the left and superior frontal QRS axis is defined as at least a -30 degrees, during the first month of life, it is defined as less than +30 degrees.
In children, a QRS frontal axis directed to the left should be regarded with suspicion. It is often a typical marker of some congenital heart diseases, such as ostium primum atrial septal defect, complete form of atrioventricular septal defect or atrioventricular canal defect, inlet-type ventricular septal defect, atrioventricular septal defect with tetralogy of Fallot, Ebstein’s anomaly, tricuspid atresia, and univentricular heart with double inlet.
The leftward and superior QRS frontal axis can be present even in pediatric patients with structurally normal hearts, due to a delay in intraventricular conduction ( left anterior fascicular block-LAFB or LAH). So a child with a left QRS axis can have a sructurally normal heart, but this should always be confirmed by a physical examination and an echocardiogram.
TWO USEFUL ECG VIDEOS SHOWING EXAMLES :
A good video showing the basic interpretation of normal and abnormal ECG with ECG examples presented.
(From MED tube). Link :
https://www.youtube.com/watch?v=Iv_MyCAIEo0
Most Important ECG Findings in Major Diseases (from USMLEVideoLectures) Link:
CARDIOLOGY BOOK ONLINE-HOME PAGE AND TABLE OF CONTENTS
Bibliography and links
A website about the intepretation of the electrocardiogram (ECG) LINK: Clinical ECG interpretation
Price D. How to read an Electrocardiogram (ECG). Part One: Basic principles of the ECG. The normal ECG. Southern Sudan Medical Journal 2010; 3(2) 26-28
LINK: How to read an electrocardiogram (ECG). Part One
How to read an electrocardiogram (ECG). Part 2: Abnormalities of Electrical Conduction Southern Sudan Medical Journal 2010; 3(4)
LINK: http://www.southsudanmedicaljournal.com/archive/november-2010/how-to-read-an-electrocardiogram-ecg.-part-2-abnormalities-of-electrical-conduction.html
Becker DE. Fundamentals of Electrocardiography Interpretation. Anesthesia Progress. 2006;53(2):53-64. doi:10.2344/0003-3006(2006)53[53:FOEI]2.0.CO;2.
LINK: Fundamentals of Electrocardiography Interpretation
Gurm HS. The ECG in acute coronary syndromes: new tricks from an old dog. Heart 2005;91(7):851-3. Available from: http://dx.doi.org/10.1136/hrt.2004.047258
LINK: The ECG in acute coronary syndromes: new tricks from an old dog
Wellens, H. J.j. "The Electrocardiogram 102 Years After Einthoven." Circulation 2004; 109(5 : 562-64. doi:10.1161/01.cir.0000117293.30403.8f.
LINK: The Electrocardiogram 102 Years After Einthoven
Farhan H, Hassan K, Al-Belushi A, Sallam M, Al-Zakwani I. Diagnostic Value of Electrocardiographic T Wave Inversion in Lead aVL in Diagnosing Coronary Artery Disease in Patients with Chronic Stable Angina. Oman Med 2010 ; 25(2): 124–127.
LINK: Diagnostic Value of Electrocardiographic T Wave Inversion in Lead aVL in Diagnosing Coronary Artery Disease in Patients with Chronic Stable Angina
68 causes of T wave, ST segment abnormalities. From Healio.com
Price D. How to read an Electrocardiogram (ECG). Part One: Basic principles of the ECG. The normal ECG. Southern Sudan Medical Journal 2010; 3(2) 26-28
LINK: How to read an electrocardiogram (ECG). Part One
How to read an electrocardiogram (ECG). Part 2: Abnormalities of Electrical Conduction Southern Sudan Medical Journal 2010; 3(4)
LINK: http://www.southsudanmedicaljournal.com/archive/november-2010/how-to-read-an-electrocardiogram-ecg.-part-2-abnormalities-of-electrical-conduction.html
Becker DE. Fundamentals of Electrocardiography Interpretation. Anesthesia Progress. 2006;53(2):53-64. doi:10.2344/0003-3006(2006)53[53:FOEI]2.0.CO;2.
LINK: Fundamentals of Electrocardiography Interpretation
Gurm HS. The ECG in acute coronary syndromes: new tricks from an old dog. Heart 2005;91(7):851-3. Available from: http://dx.doi.org/10.1136/hrt.2004.047258
LINK: The ECG in acute coronary syndromes: new tricks from an old dog
Wellens, H. J.j. "The Electrocardiogram 102 Years After Einthoven." Circulation 2004; 109(5 : 562-64. doi:10.1161/01.cir.0000117293.30403.8f.
LINK: The Electrocardiogram 102 Years After Einthoven
Farhan H, Hassan K, Al-Belushi A, Sallam M, Al-Zakwani I. Diagnostic Value of Electrocardiographic T Wave Inversion in Lead aVL in Diagnosing Coronary Artery Disease in Patients with Chronic Stable Angina. Oman Med 2010 ; 25(2): 124–127.
LINK: Diagnostic Value of Electrocardiographic T Wave Inversion in Lead aVL in Diagnosing Coronary Artery Disease in Patients with Chronic Stable Angina
68 causes of T wave, ST segment abnormalities. From Healio.com
No comments:
Post a Comment